
Abstract
Aims
To define the contribution of chronic kidney disease (CKD) to excess mortality in patients with type 2 diabetes and identify the baseline variables associated with all-cause death in those with and without CKD using the RECursive Partitioning and Amalgamation (RECPAM) method.
Methods
This observational, longitudinal, cohort study enrolled 15,773 consecutive non-dialytic patients with type 2 diabetes in 19 Diabetes Clinics throughout Italy in 2006–2008. Based on the presence of albuminuria ≥ 30 mg day−1 and/or estimated glomerular filtration rate (eGFR) < 60 mL min−1·1.73 m−2 at baseline, patients were classified as having or not CKD. Vital status was verified on October 31, 2015 for 99.26% of patients.
Results
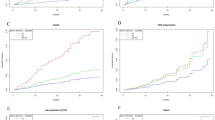
Mortality increased with increasing albuminuria and eGFR category. Excess risk versus the general population was maximal in patients aged < 55 years in the worse albuminuria or eGFR category. Conversely, in subjects aged ≥ 75 years with albuminuria < 10 mg day−1 or eGFR ≥ 75 mL min−1·1.73 m−2, excess mortality was no longer detectable. At RECPAM analysis, the main correlates of death in the whole cohort were albuminuria > 44 mg day−1, prevalent CVD, and eGFR < ~ 75 mL min−1·1.73 m−2; gender, prevalent CVD, and higher albuminuria in the normoalbuminuric range, in patients without CKD; and CVD, eGFR ~ < 50 mL min−1·1.73 m−2, and albuminuria > 53 mg day−1, in those with CKD.
Conclusions
CKD is a major contributor to excess mortality in type 2 diabetes, conferring a very high risk in younger patients and fully accounting for excess risk in the older ones. Higher albuminuria and lower eGFR, even in the normal range, identify individuals with increased mortality risk.
Trial registration ClinicalTrials.gov (NCT00715481; https://clinicaltrials.gov/ct2/show/NCT00715481).




Similar content being viewed by others

Abbreviations
- CVD:
-
Cardiovascular disease
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- CKD:
-
Chronic kidney disease
- eGFR:
-
Estimated glomerular filtration rate
- RECPAM:
-
RECursive Partitioning and Amalgamation
- RIACE:
-
Renal Insufficiency and Cardiovascular Events
- BP:
-
Blood pressure
- BMI:
-
Body mass index
- HbA1c :
-
Hemoglobin A1c
- AER:
-
Albumin excretion rate
- DR:
-
Diabetic retinopathy
- ISTAT:
-
Italian National Institute of Statistics
References
Collaboration Emerging Risk Factors, Seshasai SR, Kaptoge S et al (2011) Diabetes mellitus, fasting glucose, and risk of cause-specific death. N Engl J Med 364:829–841
Gregg EW, Cheng YJ, Saydah S et al (2012) Trends in death rates among U.S. adults with and without diabetes between 1997 and 2006: findings from the National Health Interview Survey. Diabetes Care 35:1252–1257
Preis SR, Hwang SJ, Coady S et al (2009) Trends in all-cause and cardiovascular disease mortality among women and men with and without diabetes mellitus in the Framingham Heart Study, 1950 to 2005. Circulation 119:1728–1735
Lind M, Garcia-Rodriguez LA, Booth GL et al (2013) Mortality trends in patients with and without diabetes in Ontario, Canada and the UK from 1996 to 2009: a population-based study. Diabetologia 56:2601–2608
Eliasson M, Talbäck M, Rosén M (2008) Improved survival in both men and women with diabetes between 1980 and 2004—a cohort study in Sweden. Cardiovasc Diabetol 7:32
Carstensen B, Kristensen JK, Ottosen P, Borch-Johnsen K, Steering Group of the National Diabetes Register (2008) The Danish National Diabetes Register: trends in incidence, prevalence and mortality. Diabetologia 51:2187–2196
Gulliford MC, Charlton J (2009) Is relative mortality of type 2 diabetes mellitus decreasing? Am J Epidemiol 169:455–461
Tsujimoto T, Kajio H, Sugiyama T (2018) Favourable changes in mortality in people with diabetes: US NHANES 1999–2010. Diabetes Obes Metab 20:85–93
Afkarian M, Sachs MC, Kestenbaum B et al (2013) Kidney disease and increased mortality risk in type 2 diabetes. J Am Soc Nephrol 24:302–308
Gansevoort RT, Correa-Rotter R, Hemmelgarn BR et al (2013) Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet 382:339–352
Astor BC, Hallan SI, Miller ER 3rd, Yeung E, Coresh J (2008) Glomerular filtration rate, albuminuria, and risk of cardiovascular and all-cause mortality in the US population. Am J Epidemiol 167:1226–1234
Chronic Kidney Disease Prognosis Consortium, Matsushita K, van der Velde M et al (2010) Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet 375:2073–2081
Fox CS, Matsushita K, Woodward M et al (2012) Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: a meta-analysis. Lancet 380:1662–1673
Astor BC, Matsushita K, Gansevoort RT et al (2011) Lower estimated glomerular filtration rate and higher albuminuria are associated with mortality and end-stage renal disease. A collaborative meta-analysis of kidney disease population cohorts. Kidney Int 79:1331–1340
Groop PH, Thomas MC, Moran JL et al (2009) The presence and severity of chronic kidney disease predicts all-cause mortality in type 1 diabetes. Diabetes 58:1651–1658
Orchard TJ, Secrest AM, Miller RG, Costacou T (2010) In the absence of renal disease, 20 year mortality risk in type 1 diabetes is comparable to that of the general population: a report from the Pittsburgh Epidemiology of Diabetes Complications Study. Diabetologia 53:2312–2319
de Boer IH, Katz R, Cao JJ et al (2009) Cystatin C, albuminuria, and mortality among older adults with diabetes. Diabetes Care 32:1833–1838
Ninomiya T, Perkovic V, de Galan BE et al (2009) Albuminuria and kidney function independently predict cardiovascular and renal outcomes in diabetes. J Am Soc Nephrol 20:1813–1821
Lind M, Svensson AM, Rosengren A (2015) Glycemic control and excess mortality in type 1 diabetes. N Engl J Med 372:880–881
Tancredi M, Rosengren A, Svensson AM et al (2015) Excess mortality among persons with type 2 diabetes. N Engl J Med 373:1720–1732
Penno G, Solini A, Bonora E et al (2011) Clinical significance of nonalbuminuric renal impairment in type 2 diabetes. J Hypertens 29:1802–1809
Penno G, Solini A, Bonora E et al (2013) Gender differences in cardiovascular disease risk factors, treatments and complications in patients with type 2 diabetes: the RIACE Italian multicentre study. J Intern Med 274:176–191
Pugliese G, Solini A, Fondelli C et al (2011) Reproducibility of albuminuria in type 2 diabetic subjects. Findings from the Renal Insufficiency and Cardiovascular Events (RIACE) Study. Nephrol Dial Transpl 26:3950–3954
Penno G, Solini A, Zoppini G et al (2015) Independent correlates of urinary albumin excretion within the normoalbuminuric range in patients with type 2 diabetes: the Renal Insufficiency and Cardiovascular Events (RIACE) Italian Multicentre Study. Acta Diabetol 52:971–981
Levey AS, Stevens LA, Schmid CH et al (2009) A new equation to estimate glomerular filtration rate. Ann Intern Med 150:604–612
Penno G, Solini A, Zoppini G et al (2012) Rate and determinants of association between advanced retinopathy and chronic kidney disease in patients with type 2 diabetes: the Renal Insufficiency and Cardiovascular Events (RIACE) Italian multicenter study. Diabetes Care 35:2317–2323
Solini A, Penno G, Bonora E et al (2012) Diverging association of reduced glomerular filtration rate and albuminuria with coronary and noncoronary events in patients with type 2 diabetes: the Renal Insufficiency and Cardiovascular Events (RIACE) Italian Multicenter Study. Diabetes Care 35:143–149
Italian National Institute of Statistics (ISTAT) Life tables of the residents in Italy, 2006–2015. http://demo.istat.it/tvm2016/index.php?lingua=eng. Last accessed 6 Sept 2017
Ciampi A, Hogg SA, McKinney S, Thiffault J (1988) RECPAM: a computer program for recursive partition and amalgamation for censored survival data and other situations frequently occurring in biostatistics. I. Methods and program features. Comput Methods Programs Biomed 26:239–256
Nitsch D, Grams M, Sang Y et al (2013) Associations of estimated glomerular filtration rate and albuminuria with mortality and renal failure by sex: a meta-analysis. BMJ 346:f324
Gerstein HC, Mann JF, Yi Q et al (2001) Albuminuria and risk of cardiovascular events, death, and heart failure in diabetic and nondiabetic individuals. JAMA 286:421–426
Hillege HL, Fidler V, Diercks GF et al (2002) Urinary albumin excretion predicts cardiovascular and noncardiovascular mortality in general population. Circulation 106:1777–1782
Blecker S, Matsushita K, Köttgen A et al (2011) High-normal albuminuria and risk of heart failure in the community. Am J Kidney Dis 58:47–55
Wachtell K, Ibsen H, Olsen MH et al (2003) Albuminuria and cardiovascular risk in hypertensive patients with left ventricular hypertrophy: the LIFE study. Ann Intern Med 139:901–906
Acknowledgements
This research was supported by the Research Foundation of the Italian Diabetes Society (Diabete Ricerca) and the Diabetes, Endocrinology and Metabolism (DEM) Foundation, and by unconditional grants from Eli Lilly, Sigma-Tau, Takeda, Chiesi Farmaceutici, and Boehringer Ingelheim.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
Dr. Penno reported receiving personal fees from Astra-Zeneca, Boehringer Ingelheim, Eli Lilly, and Merck Sharp & Dohme. Dr. Solini reported receiving grant from Astra-Zeneca and personal fees from Boehringer Ingelheim and Eli Lilly. Dr. Bonora reported receiving grants from Astra-Zeneca, Novo Nordisk, Roche, and Takeda and personal fees from Abbot, Astra-Zeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, Janssen, Merck Sharp & Dohme, Novo Nordisk, Roche, Sanofi-Aventis, and Takeda. Dr. Orsi reported personal fees from Abbot, Astra-Zeneca, Boehringer Ingelheim, Eli Lilly, Lifescan, Novo Nordisk, Sanofi-Aventis, and Takeda. Dr. Trevisan reported receiving personal fees from Astra-Zeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Medtronic, Novartis, Novo Nordisk, and Sanofi-Aventis and grants from Astra-Zeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Novo Nordisk, and Sanofi-Aventis. Dr. Cavalot reported receiving personal fees from Astra-Zeneca, Sanofi-Aventis, and Takeda. Dr. Nicolucci reported receiving grants from Artsana, Astra-Zeneca, Eli Lilly, Novo Nordisk, and Sanofi-Aventis and personal fees from Eli Lilly and Novo Nordisk. Dr. Pugliese reported receiving personal fees from Astra-Zeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Mylan, Shire, Sigma-Tau, and Takeda. No other disclosures were reported.
Ethical standard
The study was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments. The study protocol was approved by the locally appointed ethics committees.
Informed consent
Informed consent was obtained from all patients for being included in the study.
Additional information
Managed by Massimo Porta.
A complete list of the RIACE Investigators can be found in the Online-only Supplementary Materials.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Penno, G., Solini, A., Bonora, E. et al. Defining the contribution of chronic kidney disease to all-cause mortality in patients with type 2 diabetes: the Renal Insufficiency And Cardiovascular Events (RIACE) Italian Multicenter Study. Acta Diabetol 55, 603–612 (2018). https://doi.org/10.1007/s00592-018-1133-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00592-018-1133-z