
Abstract
Purpose
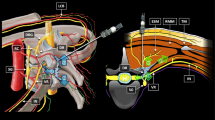
Quadratus lumborum (QL) block has four approaches. However, there is difference between the four approaches regarding efficacy, safety and adverse effects. The primary objective of this study is to compare the analgesic effect between trans-muscular and intra-muscular approaches of the QL block in pediatric patients for elective lower abdominal surgery.
Methods
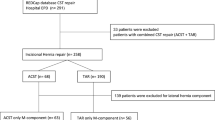
54 patients aged between 1 and 6 years were enrolled. Patients of both genders were selected. The patients were randomly classified into two groups: Group TQL includes patients (27 patients) in whom bilateral QL block was performed using trans-muscular approach, and Group IQL (27 patients), which underwent bilateral QL block using an intra-muscular approach. The primary outcome measure was the number of patients who require rescue analgesia in the first 24 h. The secondary outcome measures were FLACC score, heart rate, non-invasive blood pressure at 2, 4, 6, 12, and 24 h postoperatively, and postoperative complications (e.g., quadriceps muscle weakness, local hematoma).
Results
In the first 24 h after surgery, 13 patients in the IQL group (48.1%) required rescue analgesia, whereas only five patients in the TQL group (18.5%) required rescue analgesia. The FLACC score was lower in the TQL group than the IQL group at all time intervals up to 24 h postoperatively. In the TQL group, eight patients (29.6%) developed quadriceps weakness; whereas, only one patient (3.7%) in the IQL group developed quadriceps weakness.
Conclusion
TQL is better than IQL in the analgesic efficacy following the pediatric lower laparotomy.


Similar content being viewed by others

References
Kadam VR. Ultrasound-guided quadratus lumborum block as a postoperative analgesic technique for laparotomy. J Anaesthesiol Clin Pharmacol. 2013;29:550–52.
Blanco R. TAP block under ultrasound guidance. the description of a ‘non-pops technique’. Reg Anesth Pain Med. 2007;32:130.
Dam M, Hansen CK, Børglum J, Chan V, Bendtsen TF. A transverse oblique approach to the transmuscular quadratus lumborum block. Anesthesia. 2016;71:603–4.
Elsharkawy H. Quadratus lumborum block with paramedian sagittal oblique (subcostal) approach. Anesthesia. 2016;71:241–2.
Murouchi T. Quadratus lumborum block intramuscular approach for pediatric surgery. Acta Anesthesiol Taiwan. 2016;54:135–36.
Ueshima H, Hiroshi O. Incidence of lower-extremity muscle weakness after quadratus lumborum block. J Clin Anesth. 2018;44:104.
Ueshima H, Otake H, Lin JA. Ultrasound-guided quadratus lumborum block: an updated review of anatomy and techniques. Biomed Res Int 2017; 2017:2752876.
Wikner M. Unexpected motor weakness following quadratus lumborum block for gynecological laparoscopy. Anesthesia. 2017;72:230–2.
Merkel SI, Voepel-Lewis T, Shayevitz JR, Malviya S. The FLACC: a behavioral scale for scoring postoperative pain in young children. Pediatr Nurs. 1997;23:293–7.
Öksüz G, Bilal B, Gürkan Y, Urfalioğlu A, Arslan M, Gişi G, Öksüz H. Quadratus lumborum block versus transversus abdominis plane block in children undergoing low abdominal surgery: a randomized controlled trial. Reg Anesth Pain Med. 2017;42:674–79.
Paternostro-Sluga T, Grim-Stieger M, Posch M, Schuhfried O, Vacariu G, Mittermaier C, Bittner C, Fialka-Moser V. Reliability and validity of the Medical Research Council (MRC) scale and a modified scale for testing muscle strength in patients with radial palsy. J Rehabil Med. 2008;40:665–71.
Saito T, Den S, Tanuma K, Tanuma Y, Carney E, Carlsson C. Anatomical basis for paravertebral anesthetic block: fluid communication between the thoracic and lumbar paravertebral regions. Surg Radiol Anat. 1999;21:359–63.
Adhikary SD, El-Boghdadly K, Nasralah Z, Sarwani N, Nixon AM, Chin KJ. A radiologic and anatomic assessment of injectate spread following transmuscular quadratus lumborum block in cadavers. Anesthesia. 2017;72:73–9.
Van den Berg F, Cabri J. Applied physiology. In: Understanding and influencing the connective tissue of the musculoskeletal system. Stuttgart: Georg Thieme Publisher; 1999.
Coote JH, Perez-Gonzalez JF. The response of some sympathetic neurons to volleys in various afferent nerves. J Physiol. 1970;208:261–78.
Sauter AR, Strid JMC, Ullensvang K, Andersen MN, Daugaard M, Bendtsen MAF, Søballe K, Pedersen EM, Børglum J, Bendtsen TF. Ultrasound-guided lumbar plexus block in volunteers; a randomized controlled trial. Br J Anesth. 2017;118:430–38.
Kirchmair L, Entner T, Kapral S, Mitterschiffthaler G. Ultrasound guidance for the psoas compartment block: an imaging study. Anesth Analg. 2002;94:706–10.
Parras T, Blanco R. Randomized trial comparing the transversus abdominis plane block posterior approach or quadratus lumborum block type I with femoral block for postoperative analgesia in femoral neck fracture, both ultrasound-guided. Rev Esp Anestesiol Reanim. 2016;63:141–8.
Chakraborty A, Goswami J, Patro V. Ultrasound-guided continuous quadratus lumborum block for postoperative analgesia in a pediatric patient. A Case Rep. 2015;4:34–6.
Baidya DK, Maitra S, Arora MK, Agarwal A. Quadratus lumborum block: an effective method of perioperative analgesia in children undergoing pyeloplasty. J Clin Anesth. 2015;27:694–6.
Murouchi T, Iwasaki S, Yamakage M. Quadratus lumborum block: analgesic effects and chronological ropivacaine concentrations after laparoscopic surgery. Reg Anesth Pain Med. 2016;41:146–50.
Acknowledgements
I would like to acknowledge Dr. Mohamed Saied for the great help in postoperative data collection.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Hussein, M.M. Ultrasound-guided quadratus lumborum block in pediatrics: trans-muscular versus intra-muscular approach. J Anesth 32, 850–855 (2018). https://doi.org/10.1007/s00540-018-2563-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-018-2563-z