
Abstract
Background
Patients with branch duct type intraductal papillary mucinous neoplasm (BD-IPMN) without invasion usually show favorable prognosis. However, the prognosis becomes poor when the IPMN lesions give rise to invasive carcinoma cells. In addition, recent studies have revealed that BD-IPMN is frequently complicated by common type pancreatic ductal carcinoma. Thus, the prognosis of BD-IPMN depends on the occurrence of these two types of invasive carcinoma. However, little is known about the risk factors for the development of these invasive carcinomas in BD-IPMN. This study aims to identify the factors which predict the development of invasive carcinoma in BD-IPMN.
Methods
Invasive pancreatic carcinoma associating with BD-IPMN was classified as invasive IPMN group (invasive carcinoma derived directly from IPMN lesions) and concomitant group (common type of invasive carcinoma concomitant with BD-IPMN). The relation between the incidence of each type of invasive carcinoma in BD-IPMN and the clinicopathological parameters was retrospectively analyzed.
Results
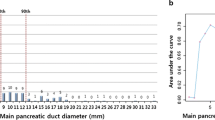
There were 12 patients with invasive IPMN and 7 patients with concomitant cancer in 159 patients with BD-IPMN. Diameter of dilated branch (P < 0.001) or main pancreatic duct (MPD) (P = 0.001), size of mural nodule (P < 0.001), serum CEA level (P < 0.001) and serum CA19-9 level (P < 0.001) were factors associated significantly with invasive IPMN by univariate analysis. Among these factors, mural nodule with size larger than 6.5 mm [odds ratio 14.86 (95% CI 1.37–60.45); P = 0.02] and serum carcinoembryonic antigen (CEA) level over 5 ng/ml [odds ratio 6.91 (95% CI 1.17–54.13); P = 0.03] were found to be the factors independently associated with invasive IPMN. On the other hand, both univariate and multivariate analyses revealed that elevated carbohydrate antigen 19-9 (CA 19-9) levels were associated with the occurrence of concomitant ductal carcinoma in BD-IPMN [odds ratio 10.31 (95% CI 1.77–81.51); P = 0.01].
Conclusions
Our results suggested that careful imaging study of the entire pancreas in addition to tumor lesions and measurement of serum CEA and CA19-9 would be required to find out the development of the two types of invasive carcinoma in BD-IPMN.



Similar content being viewed by others


Abbreviations
- IPMN:
-
Intraductal papillary mucinous neoplasms
- BD-IPMN:
-
Branch duct type intraductal papillary mucinous neoplasms
- CEA:
-
Carcinoembryonic antigen
- CA19-9:
-
Carbohydrate antigen 19-9
- EUS:
-
Endoscopic ultrasonography
- CT:
-
Computed tomography
- MRI:
-
Magnet resonance imaging
- ERCP:
-
Endoscopic retrograde cholangiopancreatography
- MPD:
-
Main pancreatic duct
References
Ohhashi K, Murakami Y, Maruyama M, Takekoshi T, Ohta H, Ohhashi I. Four cases of mucus-secreting pancreatic cancer (in Japanese). Prog Dig Endosc. 1982;20:348–51.
Kloppel G, Solicia E, Longbecker D. Histological classification of tumors of the exocrine pancreas. New York, NY: Springer Verlag; 1996.
Kobari M, Egawa S, Shibuya K, Shimamura H, Sunamura M, Takeda K, et al. Intraductal papillary mucinous tumors of the pancreas comprise 2 clinical subtypes: Differences in clinical characteristics and surgical management. Arch Surg. 1999;134:1131–6.
Terris B, Ponsot P, Paye F, Hammel P, Sauvanet A, Molas G, et al. Intraductal papillary mucinous tumors of the pancreas confined to secondary ducts show less aggressive pathologic features as compared with those involving the main pancreatic duct. Am J Surg Pathol. 2000;24:1372–7.
Doi R, Fujimoto K, Wada M, Imamura M. Surgical management of intraductal papillary mucinous tumor of the pancreas. Surgery. 2002;132:80–5.
Matsumoto T, Aramaki M, Yada K, Hirano S, Himeno Y, Shibata K, et al. Optimal management of the branch duct type intraductal papillary mucinous neoplasms of the pancreas. J Clin Gastroenterol. 2003;36:261–5.
Choi BS, Kim TK, Kim AY, Kim KW, Park SW, Kim PN, et al. Differential diagnosis of benign and malignant intraductal papillary mucinous tumors of the pancreas: MR cholangiopancreatography and MR angiography. Korean J Radiol. 2003;4:157–62.
Kitagawa Y, Unger TA, Taylor S, Kozarek RA, Traverso LW. Mucus is a predictor of better prognosis and survival in patients with intraductal papillary mucinous tumor of the pancreas. J Gastrointest Surg. 2003;7:12–8 (discussion 18–19).
Sugiyama M, Izumisato Y, Abe N, Masaki T, Mori T, Atomi Y. Predictive factors for malignancy in intraductal papillary-mucinous tumours of the pancreas. Br J Surg. 2003;90:1244–9.
Sohn TA, Yeo CJ, Cameron JL, Hruban RH, Fukushima N, Campbell KA, et al. Intraductal papillary mucinous neoplasms of the pancreas: an updated experience. Ann Surg. 2004;239:788–97 (discussion 797–789).
Salvia R, Fernandez-del Castillo C, Bassi C, Thayer SP, Falconi M, Mantovani W, et al. Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection. Ann Surg. 2004;239:678–85 (discussion 685–677).
Tanaka M, Chari S, Adsay V, et al. International consensus guideline for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology. 2006;6:17–32.
Yamao K, Ohashi K, Nakamura T, Suzuki T, Shimizu Y, Nakamura Y, et al. The prognosis of intraductal papillary mucinous tumors of the pancreas. Hepatogastroenterology. 2000;47:1129–34.
Sohn TA, Yeo CJ, Cameron JL, Iacobuzio-Donahue CA, Hruban RH, Lillemoe KD. Intraductal papillary mucinous neoplasms of the pancreas: an increasingly recognized clinicopathologic entity. Ann Surg. 2001;234:313–21 (discussion 321–312).
Raimondo M, Tachibana I, Urrutia R, Burgart LJ, DiMagno EP. Invasive cancer and survival of intraductal papillary mucinous tumors of the pancreas. Am J Gastroenterol. 2002;97:2553–8.
Chari ST, Yadav D, Smyrk TC, DiMagno EP, Miller LJ, Raimondo M, et al. Study of recurrence after surgical resection of intraductal papillary mucinous neoplasm of the pancreas. Gastroenterology. 2002;123:1500–7.
Maire F, Hammel P, Terris B, Paye F, Scoazec JY, Cellier C, et al. Prognosis of malignant intraductal papillary mucinous tumours of the pancreas after surgical resection. Comparison with pancreatic ductal adenocarcinoma. Gut. 2002;51:717–22.
Nakagohri T, Konishi M, Inoue K, Tanizawa Y, Kinoshita T. Invasive carcinoma derived from intraductal papillary mucinous carcinoma of the pancreas. Hepatogastroenterology. 2004;51:1480–3.
Suzuki Y, Atomi Y, Sugiyama M, Isaji S, Inui K, Kimura W, et al. Cystic neoplasm of the pancreas: a japanese multiinstitutional study of intraductal papillary mucinous tumor and mucinous cystic tumor. Pancreas. 2004;28:241–6.
Z’Graggen K, Rivera JA, Compton CC, Pins M, Werner J, Fernandez-del Castillo C, et al. Prevalence of activating K-ras mutations in the evolutionary stages of neoplasia in intraductal papillary mucinous tumors of the pancreas. Ann Surg. 1997;226:491–8 (discussion 498–500).
Longnecker DS. Observations on the etiology and pathogenesis of intraductal papillary-mucinous neoplasms of the pancreas. Hepatogastroenterology. 1998;45:1973–80.
Yamaguchi K, Ogawa Y, Chijiiwa K, Tanaka M. Mucin-hypersecreting tumors of the pancreas: assessing the grade of malignancy preoperatively. Am J Surg. 1996;171:427–31.
Cellier C, Cuillerier E, Palazzo L, Rickaert F, Flejou JF, Napoleon B, et al. Intraductal papillary and mucinous tumors of the pancreas: accuracy of preoperative computed tomography, endoscopic retrograde pancreatography and endoscopic ultrasonography, and long-term outcome in a large surgical series. Gastrointest Endosc. 1998;47:42–9.
Kimura W, Sasahira N, Yoshikawa T, Muto T, Makuuchi M. Duct-ectatic type of mucin producing tumor of the pancreas—new concept of pancreatic neoplasia. Hepatogastroenterology. 1996;43:692–709.
Yamaguchi K, Ohuchida J, Ohtsuka T, Nakano K, Tanaka M. Intraductal papillary-mucinous tumor of the pancreas concomitant with ductal carcinoma of the pancreas. Pancreatology. 2002;2:484–90.
Tada M, Kawabe T, Arizumi M, Togawa O, Matsubara S, Yamamoto N, et al. Pancreatic cancer in patients with pancreatic cystic lesions: a prospective study in 197 patients. Clin Gastroenterol Hepatol. 2006;4:1265–70.
Uehara H, Nakaizumi A, Ishikawa O, Iishi H, Tatsumi K, Takakura R, et al. Development of ductal carcinoma of the pancreas during follow-up of branch duct intraductal papillary mucinous neoplasm of the pancreas. Gut. 2008;57:1561–5.
Sessa F, Solcia E, Capella C, Bonato M, Scarpa A, Zamboni G, et al. Intraductal papillary-mucinous tumours represent a distinct group of pancreatic neoplasms: An investigation of tumour cell differentiation and K-ras, p53 and c-erbB-2 abnormalities in 26 patients. Virchows Arch. 1994;425:357–67.
Yamada M, Kozuka S, Yamao K, Nakazawa S, Naitoh Y, Tsukamoto Y. Mucin-producing tumor of the pancreas. Cancer. 1991;68:159–68.
Nagai E, Ueki T, Chijiiwa K, Tanaka M, Tsuneyoshi M. Intraductal papillary mucinous neoplasms of the pancreas associated with so-called “Mucinous ductal ectasia”. Histochemical and immunohistochemical analysis of 29 cases. Am J Surg Pathol. 1995;19:576–89.
Milchgrub S, Campuzano M, Casillas J, Albores-Saavedra J. Intraductal carcinoma of the pancreas. Cancer. 1992;69:651–6.
Schmidt CM, White PB, Waters JA, Yiannoutsos CT, Cummings OW, Baker M, et al. Intraductal papillary mucinous neoplasms: predictors of malignant and invasive pathology. Ann Surg. 2007;246:644–51 (discussion 651–644).
Ogawa H, Itoh S, Ikeda M, Suzuki K, Naganawa S. Intraductal papillary mucinous neoplasm of the pancreas: assessment of the likelihood of invasiveness with multisection CT. Radiology. 2008;248:876–86.
Tanno S, Nakano Y, Nishikawa T, Nakamura K, Sasajima J, Minoguchi M, et al. Natural history of branch duct intraductal papillary-mucinous neoplasms of the pancreas without mural nodules: long-term follow-up results. Gut. 2008;57:339–43.
Tang RS, Weinberg B, Dawson DW, et al. Evaluation of the guideline for management of pancreatic branch-duct intraductal papillary mucinous neoplasm. Clin Gastroenterol Hepatol. 2008;6:815–9.
Pelaez-Luna M, Chari ST, Smyrk TC, et al. Do consensus indicaions for resection in branch duct intraductal papillary mucinous neoplasm. Am J Gastroenterol. 2007;102:1759–64.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kanno, A., Satoh, K., Hirota, M. et al. Prediction of invasive carcinoma in branch type intraductal papillary mucinous neoplasms of the pancreas. J Gastroenterol 45, 952–959 (2010). https://doi.org/10.1007/s00535-010-0238-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-010-0238-0