
Abstract
Background
Gallbladder cancer (GBC) has been contraindicated for laparoscopic surgery since this procedure was introduced [1, 2]. Recently, however, there have been several reports of laparoscopic extended cholecystectomy for GBC, but most cases involved early GBC confined to the GB [3, 4]. This video describes our technique of laparoscopic extended cholecystectomy for T3 GBC.
Methods
A 77-year-old female presented with a gallbladder mass, which was incidentally detected during evaluation of back pain. Abdominal computed tomography and endoscopic ultrasonography revealed a 3.5 × 2.5 cm hypoechoic mass in the gallbladder fundus with liver invasion. We performed laparoscopic en bloc resection of the gallbladder and the gallbladder bed, as well as lymphadenectomy.
Results
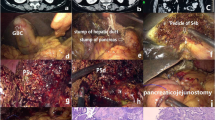
Two 5-mm and three 12-mm trocars were used. After carefully dissecting Calot’s triangle, the cystic duct was dissected and ligated. The cystic duct margin was negative on the frozen section biopsy. Cholecystectomy with en bloc wedge resection of the liver was performed first. Ultrasonic shears were used to transect the superficial hepatic parenchyma and a Cavitron Ultrasonic Surgical Aspirator was used to transect the deeper parenchyma. We then performed lymphadenectomy of involved lymph nodes (LNs) around the hepatoduodenal ligament, common hepatic artery, and posterior superior pancreas. After Kocherization of the duodenum, LNs were dissected from the posterior superior portion of the pancreas. LN dissection continued along the right side of the common bile duct and the portal vein. After dissection from the inferior vena cava and the aorta, the dissected LNs were pushed toward the left side under the portal vein. LN dissection continued along the left side of the hepatoduodenal ligament, while exposing the common hepatic artery and proper hepatic artery. Skeletonizing en bloc LN dissection was the final procedure. The operation time was 215 min and the estimated intraoperative blood loss was 200 mL. The postoperative pathology confirmed a small cell neuroendocrine carcinoma with clear resection margins. The pathologic staging was pT3N1. LN metastasis was found in one of 12 retrieved LNs. The patient was discharged on postoperative day 4 without postoperative complications. The patient received combined chemoradiation therapy for 6 months after surgery. There was no evidence of recurrence over the follow-up period of 14 months.
Conclusion
Laparoscopic extended cholecystectomy is technically feasible in patients with T3 GBC, and the extent of resection is the same as that of open surgery.
Similar content being viewed by others


References
Fong Y, Brennan MF, Turnbull A, Colt DG, Blumgart LH (1993) Gallbladder cancer discovered during laparoscopic surgery. Potential for iatrogenic tumor dissemination. Arch Surg 128(9):1054–1056
Steinert R, Nestler G, Sagynaliev E, Muller J, Lippert H, Reymond MA (2006) Laparoscopic cholecystectomy and gallbladder cancer. J Surg Oncol 93(8):682–689
de Aretxabala X, Leon J, Hepp J, Maluenda F, Roa I (2010) Gallbladder cancer: role of laparoscopy in the management of potentially resectable tumors. Surg Endosc 24(9):2192–2196
Yoon YS, Han HS, Cho JY, Choi Y, Lee W, Jang JY et al (2015) Is laparoscopy contraindicated for gallbladder cancer? A 10-year prospective cohort study. J Am Coll Surg 221(4): 847–853
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Sungho Kim, Yoo-Seok Yoon, Ho-Seong Han, Jai Young Cho, YoungRok Choi have no conflict of interest or financial ties to disclose.
Additional information
Presented at the SAGES 2017 Annual Meeting, March 22–25, 2017, Houston, TX.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary material 1 (MOV 223102 KB)
Rights and permissions
About this article

Cite this article
Kim, S., Yoon, YS., Han, HS. et al. Laparoscopic extended cholecystectomy for T3 gallbladder cancer. Surg Endosc 32, 2984–2985 (2018). https://doi.org/10.1007/s00464-017-5952-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-017-5952-8