
Abstract
Background
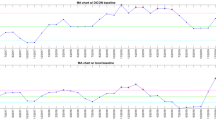
Unexpected variations in postoperative length of stay (LOS) negatively impact resources and patient outcomes. Statistical process control (SPC) measures performance, evaluates productivity, and modifies processes for optimal performance. The goal of this study was to initiate SPC to identify LOS outliers and evaluate its feasibility to improve outcomes in colorectal surgery.
Methods
Review of a prospective database identified colorectal procedures performed by a single surgeon. Patients were grouped into elective and emergent categories and then stratified by laparoscopic and open approaches. All followed a standardized enhanced recovery protocol. SPC was applied to identify outliers and evaluate causes within each group.
Results
A total of 1294 cases were analyzed—83 % elective (n = 1074) and 17 % emergent (n = 220). Emergent cases were 70.5 % open and 29.5 % laparoscopic; elective cases were 36.8 % open and 63.2 % laparoscopic. All groups had a wide range in LOS. LOS outliers ranged from 8.6 % (elective laparoscopic) to 10.8 % (emergent laparoscopic). Evaluation of outliers demonstrated patient characteristics of higher ASA scores, longer operating times, ICU requirement, and temporary nursing at discharge. Outliers had higher postoperative complication rates in elective open (57.1 vs. 20.0 %) and elective lap groups (77.6 vs. 26.1 %). Outliers also had higher readmission rates for emergent open (11.4 vs. 5.4 %), emergent lap (14.3 vs. 9.2 %), and elective lap (32.8 vs. 6.9 %). Elective open outliers did not follow trends of longer LOS or higher reoperation rates.
Conclusions
SPC is feasible and promising for improving colorectal surgery outcomes. SPC identified patient and process characteristics associated with increased LOS. SPC may allow real-time outlier identification, during quality improvement efforts, and reevaluation of outcomes after introducing process change. SPC has clinical implications for improving patient outcomes and resource utilization.


Similar content being viewed by others

References
Fearon KC, Ljungqvist O, Von Meyenfeldt M et al (2005) Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr 24:466–477
Wind J, Polle SW, Fung Kon Jin PH et al (2006) Systematic review of enhanced recovery programmes in colonic surgery. Br J Surg 93:800–809
Kehlet H, Wilmore DW (2002) Multimodal strategies to improve surgical outcome. Am J Surg 183:630–641
Wilmore DW, Kehlet H (2001) Management of patients in fast track surgery. BMJ 322:473–476
Adamina M, Kehlet H, Tomlinson GA, Senagore AJ, Delaney CP (2011) Enhanced recovery pathways optimize health outcomes and resource utilization: a meta-analysis of randomized controlled trials in colorectal surgery. Surgery 149:830–840
Delaney CP, Zutshi M, Senagore AJ, Remzi FH, Hammel J, Fazio VW (2003) Prospective, randomized, controlled trial between a pathway of controlled rehabilitation with early ambulation and diet and traditional postoperative care after laparotomy and intestinal resection. Dis Colon Rectum 46:851–859
Kehlet H, Mogensen T (1999) Hospital stay of 2 days after open sigmoidectomy with a multimodal rehabilitation programme. Br J Surg 86:227–230
Kehlet H, Wilmore DW (2008) Evidence-based surgical care and the evolution of fast-track surgery. Ann Surg 248:189–198
Kehlet H (2008) Fast-track colorectal surgery. Lancet 371:791–793
Collins TC, Daley J, Henderson WH, Khuri SF (1999) Risk factors for prolonged length of stay after major elective surgery. Ann Surg 230:251–259
Nicolay CR, Purkayastha S, Greenhalgh A et al (2012) Systematic review of the application of quality improvement methodologies from the manufacturing industry to surgical healthcare. Br J Surg 99:324–335
Deming WE (1990) Some notes on management in a hospital. J Soc Health Syst 2:74–77
Mohammed MA (2004) Using statistical process control to improve the quality of health care. Qual Saf Health Care 13:243–245
Deming WE (1980) The statistical procedure in the SENIC Project. Am J Epidemiol 111:470–471
Shewhart WA (1922) On the measurement of a physical quantity whose magnitude is influenced by primary causes beyond the control of the observer and on the method of determining the relation between two such quantities. Proc Natl Acad Sci USA 8:248–251
Sedlack JD (2010) The utilization of six sigma and statistical process control techniques in surgical quality improvement. J Healthc Qual 32:18–26
NIST/SEMATECH e-Handbook of statistical method. 2012; 6.1.2. What are process control techniques? <http://www.itl.nist.gov/div898/handbook/pmc/section1/pmc12.htm>
Delaney CP (2008) Outcome of discharge within 24 to 72 hours after laparoscopic colorectal surgery. Dis Colon Rectum 51:181–185
Delaney CP, Brady K, Woconish D, Parmar SP, Champagne BJ (2012) Towards optimizing perioperative colorectal care: outcomes for 1,000 consecutive laparoscopic colon procedures using enhanced recovery pathways. Am J Surg 203:353–355 discussion 355–6
Kim CS, Spahlinger DA, Kin JM, Billi JE (2006) Lean health care: what can hospitals learn from a world-class automaker? J Hosp Med 1:191–199
Fry DE, Pine M, Jones BL, Meimban RJ (2011) The impact of ineffective and inefficient care on the excess costs of elective surgical procedures. J Am Coll Surg 212:779–786
Curran ET, Benneyan JC, Hood J (2002) Controlling methicillin-resistant Staphylococcus aureus: a feedback approach using annotated statistical process control charts. Infect Control Hosp Epidemiol 23:13–18
Ryckman FC, Schoettker PJ, Hays KR et al (2009) Reducing surgical site infections at a pediatric academic medical center. Jt Comm J Qual Patient Saf 35:192–198
Duclos A, Touzet S, Soardo P, Colin C, Peix JL, Lifante JC (2009) Quality monitoring in thyroid surgery using the Shewhart control chart. Br J Surg 96:171–174
Chen TT, Chang YJ, Ku SL, Chung KP (2010) Statistical process control as a tool for controlling operating room performance: retrospective analysis and benchmarking. J Eval Clin Pract 16:905–910
Keller DS, Stulberg JJ, Lawrence JK, Delaney CP (2014) Process control to measure process improvement in colorectal surgery: modifications to an established enhanced recovery pathway. Dis Colon Rectum 57:194–200
Disclosures
Drs. Deborah S. Keller, Jonah J. Stulberg, Justin K. Lawrence, Hoda Samia, and Conor P. Delaney have no conflicts of interest and nothing to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Keller, D.S., Stulberg, J.J., Lawrence, J.K. et al. Initiating statistical process control to improve quality outcomes in colorectal surgery. Surg Endosc 29, 3559–3564 (2015). https://doi.org/10.1007/s00464-015-4108-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-015-4108-y