
Abstract
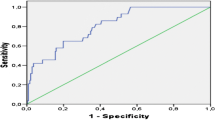
Diagnosing a urinary tract infection in children is often difficult due to non-specific symptoms and requires invasive and time-consuming procedures. Flow cytometry is a new and rapid method of analyzing urine to confirm or exclude UTIs. We have investigated the sensitivity and specificity of urine flow cytometry (Sysmex UF1000i) compared to conventional diagnostic techniques in a prospective study from January 1, 2014 until January 1, 2015. All children under 13 years of age with a suspicion of urinary tract infection were screened using both urine flow cytometry and urine culture. A urinary tract infection was defined as the combination of leukocyturia (≥ 25 leukocytes per μl) and a positive urine culture in the presence of clinical symptoms. A total number of 412 urine samples were collected, of which 63 cases (15.3%) were positive for a urinary tract infection. Receiver operating characteristic analysis showed an area under the curve of 0.97 (95% confidence interval h0.93–1.00) for the bacterial count. When using a cut-off value of 250 bacteria/μl in the presence of leukocyturia, the sensitivity for urinary tract infection is 0.97 with a negative predictive value of 97%, and the specificity is 0.91 with a positive predictive value of 90%.
Conclusion: Flow cytometry–based bacterial and leukocyte count analysis is a time-efficient method of diagnosing or ruling out urinary tract infection in children, with a higher sensitivity and specificity than dipstick and microscopic analysis.
What is known • Screening for urinary tract infections in children is difficult due to invasive and time-consuming procedures. • There is both over- and under-treatment of urinary tract infections due to the delays in accurate diagnosing. | |
What is new • Flow cytometry is a rapid and accurate method to provide useful information in the diagnosis of urinary tract infection in children. When negative, flow cytometry can exclude urinary tract infection in children with a high degree of confidence. When flow cytometry is positive, the possibility of a urinary tract infection in children is increased. |


Similar content being viewed by others


Abbreviations
- AUC:
-
Area under the curve
- CFU:
-
Colony forming units
- CI:
-
Confidence interval
- ROC:
-
Receiver operating characteristic
- UTI:
-
Urinary tract infection
References
Benador D, Benador N, Slosman D, Mermillod B, Girardin E (1997) Are younger children at highest risk of renal sequelae after pyelonephritis? Lancet 349:17–19
Boonen KJ, Koldewijn EL, Arents NL, Raaymakers PA, Scharnhorst V (2013) Urine flow cytometry as a primary screening method to exclude urinary tract infections. World J Urol 31:547–551
Broeren MA, Bahceci S, Vader HL, Arents NL (2011) Screening for urinary tract infection with the Sysmex UF-1000i urine flow cytometer. J Clin Microbiol 49:1025–1029
De Rosa R, Grosso S, Bruschetta G, Avolio M, Stano P, Modolo ML, Camporese A (2010) Evaluation of the Sysmex UF1000i flow cytometer for ruling out bacterial urinary tract infection. Clin Chim Acta 411:1137–1142
Doganis D, Siafas K, Mavrikou M, Issaris G, Martirosova A, Perperidis G, Konstantopoulos A, Sinaniotis K (2007) Does early treatment of urinary tract infection prevent renal damage? Pediatrics 120:e922–e928
Duong HP, Wissing KM, Tram N, Mascart G, Lepage P, Ismaili K (2016) Accuracy of automated flow cytometry-based leukocyte counts to rule out urinary tract infection in febrile children: a prospective cross-sectional study. J Clin Microbiol 54:2975–2981
Giesen CD, Greeno AM, Thompson KA, Patel R, Jenkins SM, Lieske JC (2013) Performance of flow cytometry to screen urine for bacteria and white blood cells prior to urine culture. Clin Biochem 46:810–813
Hellerstein S (1982) Recurrent urinary tract infections in children. Pediatr Infect Dis 1:271–281
Hoberman A, Chao HP, Keller DM, Hickey R, Davis HW, Ellis D (1993) Prevalence of urinary tract infection in febrile infants. J Pediatr 123:17–23
Hoberman A, Wald ER, Reynolds EA, Penchansky L, Charron M (1994) Pyuria and bacteriuria in urine specimens obtained by catheter from young children with fever. J Pediatr 124:513–519
Jakobsson B, Svensson L (1997) Transient pyelonephritic changes on 99mTechnetium-dimercaptosuccinic acid scan for at least five months after infection. Acta Paediatr 86:803–807
Kanegaye JT, Jacob JM, Malicki D (2014) Automated urinalysis and urine dipstick in the emergency evaluation of young febrile children. Pediatrics 134:523–529
Le Z, Li F, Fei C, Ye A, Xie X, Zhang J (2016) Performance of the Sysmex UF-1000i urine analyser in the rapid diagnosis of urinary tract infections in hospitalized patients. J Infect Chemother 22:377–382
Lin DS, Huang SH, Lin CC, Tung YC, Huang TT, Chiu NC, Koa HA, Hung HY, Hsu CH, Hsieh WS, Yang DI, Huang FY (2000) Urinary tract infection in febrile infants younger than eight weeks of age. Pediatrics 105:E20
Luco M, Lizama M, Reichhard C, Hirsch T (2006) Urine microscopy as screen for urinary tract infections in a pediatric emergency unit in Chile. Pediatr Emerg Care 22:705–709
Manoni F, Gessoni G, Caleffi A, Alessio MG, Rosso R, Menozzi P, Tinello A, Valverde S, Azzara G, Lippi G (2013) Pediatric reference values for urine particle quantification by using automated flow cytometer: results of a multicenter study of Italian urinalysis group. Clin Biochem 46:1820–1824
Metz CE (1978) Basic principles of ROC analysis. Semin Nucl Med 8:283–298
Nederlandse Vereniging voor Kindergeneeskunde (2010) Richtlijn urineweginfecties bij kinderen [NVK web site]. Avaliable at: https://www.nvk.nl/Portals/0/richtlijnen/uwi/richtlijnuwi.pdf
Shang YJ, Wang QQ, Zhang JR, Xu YL, Zhang WW, Chen Y, Gu ML, Hu ZD, Deng AM (2013) Systematic review and meta-analysis of flow cytometry in urinary tract infection screening. Clin Chim Acta 424:90–95
Shaw KN, Gorelick M, McGowan KL, Yakscoe NM, Schwartz JS (1998) Prevalence of urinary tract infection in febrile young children in the emergency department. Pediatrics 102:e16
Subcommittee on Urinary Tract Infection, Steering Committee on Quality Improvement and Management, Roberts KB (2011) Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics 128:595–610
Zorc JJ, Levine DA, Platt SL, Dayan PS, Macias CG, Krief W, Schor J, Bank D, Shaw KN, Kuppermann N, Multicenter RSV-SBI Study Group of the Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics (2005) Clinical and demographic factors associated with urinary tract infection in young febrile infants. Pediatrics 116:644–648
Author information
Authors and Affiliations
Contributions
M. Broeren participated in the study design analysis and especially the statistical analysis, and writing the manuscript.
R. Nowacki participated in the study design analysis, patient inclusion and writing the manuscript.
F. Halbertsma participated in the study design, patient inclusion, analysis and writing the manuscript.
N. Arents participated in the micribiological analysis, and writing the manuscript.
S. Zegers participated in the study design analysis the statistical analysis, and writing the manuscript especially related to clinical relevance.
Corresponding authors
Additional information
Communicated by Mario Bianchetti
Rights and permissions
About this article

Cite this article
Broeren, M., Nowacki, R., Halbertsma, F. et al. Urine flow cytometry is an adequate screening tool for urinary tract infections in children. Eur J Pediatr 178, 363–368 (2019). https://doi.org/10.1007/s00431-018-3307-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-018-3307-7