
Abstract
Introduction
Nodular lesions within the neck may origin from several structures. A misdiagnosed origin may expose the surgeon to inappropriate procedures. These lesions are paradoxically frequent in high specialised centre for endocrine surgery.
Patients and methods
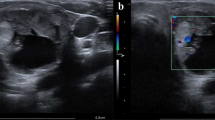
In the year 2006, three patients were first admitted to our department with a diagnosis of thyroid nodule (1) or lymphatic metastases of thyroid carcinoma (2). The first patient had ultrasound (US) and Tc-99-m scan orienting for thyroid nodule. The two other patients, presented with lateral neck lesion in ipsilateral sincronous and previous diagnosis of papillary thyroid carcinoma, respectively, with US and computed tomography scan confirmed lesion but with a FNA cytology negative for tumoural cells.
Results
All three patients underwent surgical exploration. In the first two cases, a whitish tender nodule (4 and 4.5cm), cleavable from surrounding structures, was removed with final histology of Schwannoma and Paraganglioma, respectively. Both patients experienced Bernard Horner Syndrome. In the last patients, a firm grey nodule of 5cm strictly adherent to muscular planes was removed with diagnosis of Castleman’s Disease.
Conclusions
Nodular neck lesions mimicking a thyroid pathology (thyroid nodules or metastatic lymph nodes) are rare but can represent a tough challenge for surgeons who might fall into incorrect surgical approaches, resulting in high morbidity. Pre-operative work-up would help the surgeon to obtain the correct diagnosis, thus, to follow the better surgical approach. Nevertheless, a careful approach would be used for that neurogenic tumour amenable of resection without jeopardising nervous structures.








Similar content being viewed by others

References
Leonardis M, Sperb D, Aster C, Campisi C, Herter NT (2003) Ganglioneuroma of the neck, masquerading as a goiter. Eur J Surg Oncol 29:929–930, doi:10.1016/j.ejso.2003.08.010
Mikosch P, Gallowitsch HJ, Kresnik E, Lind P (1997) Schwannoma of the neck simulating a thyroid nodule. Thyroid 7(3):449–451
Aron M, Kapila K, Verma K (2005) Neural tumours of the neck presentino as thyroid nodules: a report of three cases. Cytopathology 16:206–209, doi:10.1111/j.1365-2303.2005.00246.x
Chaloupka JC, Castillo M, Hudgins P (1990) Castleman’s disease in the neck: a typical appearance on CT. AJR Am J Roentgenol 154:1051–1052
Kooper DP, Tiwari RM, van der Valk P (1994) Castlman’s disease a san uncommon cause of a neck mass. Eur Arch Otorhinolaryngol 251:370–372, doi:10.1007/BF00171548
Sherman JA, Birtwhistle CJ, Davies HT (2001) A rapidly expanding lesion in the neck: unusual presentation of Castleman’s diesease. Int J Maxillofac Surg 30:458–460, doi:10.1054/ijom.2001.0119
Bond SE, Saeed NR, Palka I (2003) Castleman’s disease presenting as a midline neck mass. Br J Plast Surg 56:62–64, doi:10.1016/S0007-1226(02)00478-2
Denenberg S (1984) levine PA. Castleman’s disease: the lymphoma impostor. Laryngoscope 94:601–603, doi:10.1288/00005537-198405000-00003
De Paoli F, Giugliano G, Casadio C, Tredici P, Bruschini R, De Fiori E (2005) Schwannoma of thyroid bed. A case report and considerations on interdisciplinary collaboration. Acta Otorhinolaryngol Ital 25(4):250–252
Badawi RA, Scott-Coombes D (2002) Ancient schwannoma masquerading as a thyroid mass. Eur J Surg Oncol 28:88–94, doi:10.1053/ejso.2001.1159
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Donatini, G., Iacconi, P., De Bartolomeis, C. et al. Neck lesions mimicking thyroid pathology. Langenbecks Arch Surg 394, 435–440 (2009). https://doi.org/10.1007/s00423-008-0410-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-008-0410-7