
Abstract
Background
International trials suggest benefit of revascularization surgery (RS) for moyamoya disease (MMD). However, nationally representative US data on demographics and outcomes after RS in MMD are lacking.
Aims
To estimate causes and rates of readmission after RS for MMD.
Methods
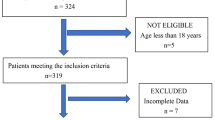
In the Nationwide Readmissions Database, index admissions for ECICB for MMD and readmissions for ischemic stroke (IS), subarachnoid hemorrhage (SAH), and intracerebral hemorrhage (ICH) were identified using validated International Classification of Diseases, Ninth Revision, Clinical Modification codes. We summarized demographics and comorbidities, and calculated 30-, 60-, and 90-day readmission rates per 100,000 index admissions.
Results
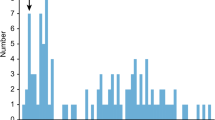
Among 201 index admissions for RS for MMD, mean age (SD) was 41.7 (12.6) years; 75% were female; 24% had diabetes; 53% had hypertension; 40% had hypercholesterolemia; 3% had ICH; 16% had IS; and 1% had SAH. RS was performed at large hospitals in 83%, urban hospitals in 85%, and teaching hospitals in 97%. 80% were discharged home. 34% had a readmission during follow-up. Leading reasons for readmission up to 90 days included MMD (62%), postoperative infection (10%), sickle cell crisis (4%), ischemic stroke (4%), epilepsy (2%), subdural hemorrhage (2%) and headache (2%). Readmission rates (per 100,000 index admissions) were 559 at 30 days, 1829 at 60 days, and 2027 at 90 days for IS. There were no readmissions for SAH or ICH.
Conclusions
This analysis of nationally representative US data suggests that although readmission after RS for MMD is not uncommon, cerebral hemorrhagic events during the 90-day postoperative period are rare.

Similar content being viewed by others

References
Arias EJ, Derdeyn CP, Dacey RG Jr, Zipfel GJ (2014) Advances and surgical considerations in the treatment of moyamoya disease. Neurosurgery 74(Suppl 1):S116–S125
Baram D, Daroowalla F, Garcia R, Zhang G, Chen JJ, Healy E et al (2008) Use of the all patient refined-diagnosis related group (APR-DRG) risk of mortality score as a severity adjustor in the medical ICU. Clin Med Circ Respir Pulm Med 2:19–25
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
de Groot V, Beckerman H, Lankhorst GJ, Bouter LM (2003) How to measure comorbidity. A critical review of available methods. J Clin Epidemiol 56:221–229
Duan L, Bao XY, Yang WZ, Shi WC, Li DS, Zhang ZS et al (2012) Moyamoya disease in China: its clinical features and outcomes. Stroke 43:56–60
Fujimura M, Tominaga T (2012) Lessons learned from moyamoya disease: outcome of direct/indirect revascularization surgery for 150 affected hemispheres. Neurol Med Chir (Tokyo) 52:327–332
Gross BA, Du R (2013) Adult moyamoya after revascularization. Acta Neurochir (Wien) 155:247–254
Guzman R, Lee M, Achrol A, Bell-Stephens T, Kelly M, Do HM et al (2009) Clinical outcome after 450 revascularization procedures for moyamoya disease. Clinical article. J Neurosurg 111:927–935
Houkin K, Nakayama N, Kuroda S, Ishikawa T, Nonaka T (2004) How does angiogenesis develop in pediatric moyamoya disease after surgery? A prospective study with MR angiography. Childs Nerv Syst 20:734–741
Imaizumi T, Hayashi K, Saito K, Osawa M, Fukuyama Y (1998) Long-term outcomes of pediatric moyamoya disease monitored to adulthood. Pediatr Neurol 18:321–325
Kainth D, Chaudhry SA, Kainth H, Suri FK, Qureshi AI (2013) Epidemiological and clinical features of moyamoya disease in the USA. Neuroepidemiology 40:282–287
Karasawa J, Kikuchi H, Furuse S, Kawamura J, Sakaki T (1978) Treatment of moyamoya disease with STA-MCA anastomosis. J Neurosurg 49:679–688
Kawaguchi S, Okuno S, Sakaki T (2000) Effect of direct arterial bypass on the prevention of future stroke in patients with the hemorrhagic variety of moyamoya disease. J Neurosurg 93:397–401
Kazumata K, Ito M, Uchino H, Nishihara H, Houkin K (2017) Proposal for a prospective registry for Moyamoya disease in Japan. Neurol Medico-Chirurgica 57:66–72
Kim T, Oh CW, Kwon OK, Hwang G, Kim JE, Kang HS et al (2016) Stroke prevention by direct revascularization for patients with adult-onset moyamoya disease presenting with ischemia. J Neurosurg 124:1788–1793
Kraemer M, Heienbrok W, Berlit P (2008) Moyamoya disease in Europeans. Stroke 39:3193–3200
Kuroda S, Ishikawa T, Houkin K, Nanba R, Hokari M, Iwasaki Y (2005) Incidence and clinical features of disease progression in adult moyamoya disease. Stroke 36:2148–2153
Lee DJ, Liebeskind DS (2011) Characterization of inpatient moyamoya in the United States: 1988–2004. Front Neurol 2:43
Miyamoto S, Yoshimoto T, Hashimoto N, Okada Y, Tsuji I, Tominaga T et al (2014) Effects of extracranial-intracranial bypass for patients with hemorrhagic moyamoya disease: results of the Japan Adult Moyamoya Trial. Stroke 45:1415–1421
Narisawa A, Fujimura M, Tominaga T (2009) Efficacy of the revascularization surgery for adult-onset moyamoya disease with the progression of cerebrovascular lesions. Clin Neurol Neurosurg 111:123–126
Parikh NS, Cool J, Karas MG, Boehme AK, Kamel H (2016) Stroke risk and mortality in patients with ventricular assist devices. Stroke 47:2702–2706
Shen Y (2003) Applying the 3M all patient refined diagnosis related groups grouper to measure inpatient severity in the VA. Med Care 41:Ii103–I110
Starke RM, Crowley RW, Maltenfort M, Jabbour PM, Gonzalez LF, Tjoumakaris SI et al (2012) Moyamoya disorder in the United States. Neurosurgery 71:93–99
Tirschwell DL, Longstreth WT Jr (2002) Validating administrative data in stroke research. Stroke 33:2465–2470
Titsworth WL, Scott RM, Smith ER (2016) National analysis of 2454 pediatric Moyamoya admissions and the effect of hospital volume on outcomes. Stroke 47:1303–1311
Uchino K, Johnston SC, Becker KJ, Tirschwell DL (2005) Moyamoya disease in Washington State and California. Neurology 65:956–958
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical standards
This research was approved by the Mount Sinai IRB ethics committee and was therefore performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
Rights and permissions
About this article

Cite this article
Kahn, A., Kaur, G., Stein, L. et al. Treatment course and outcomes after revascularization surgery for moyamoya disease in adults. J Neurol 265, 2666–2671 (2018). https://doi.org/10.1007/s00415-018-9044-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-018-9044-z