
Abstract
Introduction
Endoscopic balloon dilation (EBD) is the mainstay of endoscopic therapy for laryngotracheal stenosis (LTS), although there is no evidence that it achieves better results than traditional rigid laryngeal dilators. Rigid bougie dilators are less expensive and easier to use, and confer the advantage of providing tactile information about the stenosis to the surgeon. We analyzed the outcome of endoscopic rigid bougie dilatation of LTS in a large series of children and compared it to the reported results of EBD in the same setting.
Patients and methods
All cases of pediatric LTS treated by endoscopic rigid dilatation in a tertiary referral center between 2006 and 2015 were retrospectively studied. They were divided into a primary dilatation group (PDG) and a post-reconstruction dilatation group (PRG). The PDG children had no history of reconstructive airway surgery, and dilatation was the major treatment approach. The PRG children underwent dilatations after airway reconstruction surgery as part of routine postoperative management. A successful primary outcome was defined as improvement of dyspnea and achievement of a functional airway without reconstructive laryngotracheal surgery or need for a tracheostomy at final follow-up.
Results
Sixty-two children (68 cases, mean age 5.1 years, range 0.7–17.2) underwent 156 endoscopic rigid dilatations. Successful outcome was achieved in 48 cases (70.6%), 73.0% in the PDG and 67.7% in the PRG. There were no procedure-related adverse events.
Conclusions
Endoscopic rigid dilatation is a relatively inexpensive and efficacious tool in endoscopic management of pediatric LTS. Its success rates are in the same range as those of EBD.



Similar content being viewed by others


References
Avelino M, Maunsell R, Jube Wastowski I (2015) Predicting outcomes of balloon laryngoplasty in children with subglottic stenosis. Int J Pediatr Otorhinolaryngol 79(4):532–536. https://doi.org/10.1016/j.ijporl.2015.01.022
Durden F, Sobol SE (2007) Balloon laryngoplasty as a primary treatment for subglottic stenosis. Arch Otolaryngol Head Neck Surg 133(8):772–775. https://doi.org/10.1001/archotol.133.8.772
Guarisco JL, Yang CJ (2013) Balloon dilation in the management of severe airway stenosis in children and adolescents. J Pediatr Surg 48(8):1676–1681. https://doi.org/10.1016/j.jpedsurg.2012.12.035
Hautefort C, Teissier N, Viala P, Van Den Abbeele T (2012) Balloon dilation laryngoplasty for subglottic stenosis in children: eight years’ experience. Arch Otolaryngol Head Neck Surg 138(3):235–240. https://doi.org/10.1001/archoto.2011.1439
Maresh A, Preciado DA, O’Connell AP, Zalzal GH (2014) A comparative analysis of open surgery vs endoscopic balloon dilation for pediatric subglottic stenosis. JAMA Otolaryngol Head Neck Surg 140(10):901–905. https://doi.org/10.1001/jamaoto.2014.1742
Ortiz R, Dominguez E, De La Torre C, Hernandez F, Encinas JL, Lopez-Fernandez S, Castro L, Menendez JJ, De la Serna O, Vazquez J, Santamaria ML, Tovar JA (2014) Early endoscopic dilation and mitomycin application in the treatment of acquired tracheal stenosis. Eur J Pediatr Surg 24(1):39–45. https://doi.org/10.1055/s-0033-1357754
Wentzel JL, Ahmad SM, Discolo CM, Gillespie MB, Dobbie AM, White DR (2014) Balloon laryngoplasty for pediatric laryngeal stenosis: case series and systematic review. Laryngoscope 124(7):1707–1712. https://doi.org/10.1002/lary.24524
Whigham AS, Howell R, Choi S, Pena M, Zalzal G, Preciado D (2012) Outcomes of balloon dilation in pediatric subglottic stenosis. Ann Otol Rhinol Laryngol 121(7):442–448. https://doi.org/10.1177/000348941212100704
Bakthavachalam S, McClay JE (2008) Endoscopic management of subglottic stenosis. Otolaryngol Head Neck Surg 139(4):551–559. https://doi.org/10.1016/j.otohns.2008.07.024
Maksoud-Filho JG, Goncalves ME, Cardoso SR, Tannuri U (2008) Early diagnostic and endoscopic dilatation for the treatment of acquired upper airway stenosis after intubation in children. J Pediatr Surg 43(7):1254–1258. https://doi.org/10.1016/j.jpedsurg.2007.10.057
Pashley NR (1983) Serial dilation compared to elective laryngo-tracheoplasty in the treatment of acquired subglottic stenosis in children. Int J Pediatr Otorhinolaryngol 5(1):59–65
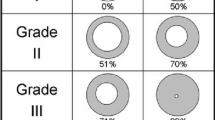
Myer CM 3rd, O’Connor DM, Cotton RT (1994) Proposed grading system for subglottic stenosis based on endotracheal tube sizes. Ann Otol Rhinol Laryngol 103(4 Pt 1):319–323
Hseu AF, Benninger MS, Haffey TM, Lorenz R (2014) Subglottic stenosis: a ten-year review of treatment outcomes. Laryngoscope 124(3):736–741. https://doi.org/10.1002/lary.24410
Brown SB, Hedlund GL, Glasier CM, Williams KD, Greenwood LH, Gilliland JD (1987) Tracheobronchial stenosis in infants: successful balloon dilation therapy. Radiology 164(2):475–478. https://doi.org/10.1148/radiology.164.2.3602388
Hebra A, Powell DD, Smith CD, Othersen HB Jr (1991) Balloon tracheoplasty in children: results of a 15-year experience. J Pediatr Surg 26(8):957–961
Modi VK, Visaya JM, Ward RF (2015) Histopathological effect of balloon dilation in a live rabbit: implications for the pediatric airway. Laryngoscope 125 (Suppl 6):S1–S11. https://doi.org/10.1002/lary.25425
Messineo A, Forte V, Joseph T, Silver MM, Filler RM (1992) The balloon posterior tracheal split: a technique for managing tracheal stenosis in the premature infant. J Pediatr Surg 27(8):1142–1144
Acknowledgements
Esther Eshkol is thanked for editorial assistance.
Funding
None. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Yafit, D., Cavel, O., Ungar, O.J. et al. Rigid dilatation of pediatric laryngotracheal stenosis as an adequate alternative to balloon dilatation. Eur Arch Otorhinolaryngol 275, 2529–2533 (2018). https://doi.org/10.1007/s00405-018-5087-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-018-5087-0