
Abstract
Background
Inspiratory strength after a neck dissection has not been evaluated, and diaphragm function has not been adequately evaluated.
Objective
Evaluate diaphragm mobility and inspiratory strength after neck dissection.
Methods
Prospective data collection of a consecutive series of adult patients submitted to neck dissection for head and neck cancer treatment, in a tertiary referral cancer center, from January to September 2014, with 30 days of follow-up. A total of 43 were studied (recruited 56; excluded 13).
Main outcome measures
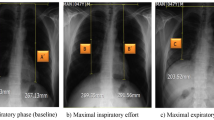
Determine diaphragm mobility and inspiratory muscle strength after neck dissection, using diaphragm ultrasound and by measuring maximal inspiratory pressure (MIP) and sniff nasal inspiratory pressure (SNIP).
Results
Thirty patients underwent unilateral neck dissection, and thirteen patients underwent bilateral neck dissection. Diaphragm immobility occurred in 8.9% of diaphragms at risk. For the entire cohort, inspiratory strength decreased immediately after the dissection but returned to preoperative values after 1 month. Except for those with diaphragm immobility, diaphragm mobility remained unchanged after the dissection. One month after the dissection, the diaphragm thickness decreased, indicating diaphragm atrophy.
Conclusions
Immediately after a neck dissection, just a few patients showed diaphragmatic immobility, and there was a transient decrease in inspiratory strength in all individuals. Such findings can increase the risk of postoperative complications in patients with previous lung disease.




Similar content being viewed by others


References
Ferlito A, Robbins KT, Shah JP, Medina JE, Silver CE, Al-Tamimi S et al (2011) Proposal for a rational classification of neck dissections. Head Neck 33:445–450
Vartanian JG, Pontes E, Agra IM, Campos OD, Goncalves-Filho J, Carvalho AL et al. (2003) Distribution of metastatic lymph nodes in oropharyngeal carcinoma and its implications for the elective treatment of the neck. Arch Otolaryngol Head Neck Surg 129:729–732
Laghi F, Tobin MJ (2003) Disorders of the respiratory muscles. Am J Respir Crit Care Med 168:10–48
McCool FD, Tzelepis GE (2012) Dysfunction of the diaphragm. N Engl J Med 366:932–942
Rochester DF, Farkas GA (1995) Performance of respiratory muscles in situ. In: Roussos C (ed) The thorax: applied physiology. Marcel Dekker, New York. 1127–1159
Siafakas NM, Mitrouska I, Bouros D, Georgopoulos D (1999) Surgery and the respiratory muscles. Thorax 54:458–465
Bergman NA, Tien YK (1983) Contribution of the closure of pulmonary units to impaired oxygenation during anesthesia. Anesthesiology 59:395–401
Shander A, Fleisher LA, Barie PS, Bigatello LM, Sladen RN, Watson CB (2011) Clinical and economic burden of postoperative pulmonary complications: patient safety summit on definition, risk-reducing interventions, and preventive strategies. Crit Care Med 39:2163–2172
de Jong AA, Manni JJ (1991) Phrenic nerve paralysis following neck dissection. European archives of oto-rhino-laryngology: official journal of the European Federation of Oto-Rhino. Laryngol Soc 248:132–134
Moorthy SS, Gibbs PS, Losasso AM, Lingeman RE (1983) Transient paralysis of the diaphragm following radical neck surgery. Laryngoscope 93:642–644
Yaddanapudi S, Shah SC (1996) Bilateral phrenic nerve injury after neck dissection: an uncommon cause of respiratory failure. J Laryngol Otol 110:281–283
Gottesman E, McCool FD (1997) Ultrasound evaluation of the paralyzed diaphragm. Am J Respir Crit Care Med 155:1570–1574
Boon AJ, Harper CJ, Ghahfarokhi LS, Strommen JA, Watson JC, Sorenson EJ (2013) Two-dimensional ultrasound imaging of the diaphragm: quantitative values in normal subjects. Muscle Nerve 47:884–889
Testa A, Soldati G, Giannuzzi R, Berardi S, Portale G, Gentiloni Silveri N (2011) Ultrasound M-mode assessment of diaphragmatic kinetics by anterior transverse scanning in healthy subjects. Ultrasound Med Biol 37:44–52
Piccirillo JF, Feinstein AR (1996) Clinical symptoms and comorbidity: significance for the prognostic classification of cancer. Cancer 77:834–842
Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET et al. (1982) Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 5:649–655
American Thoracic Society/European Respiratory S. (2002) ATS/ERS statement on respiratory muscle testing. Am J Respir Crit Care Med 166:518–624
Steier J, Kaul S, Seymour J, Jolley C, Rafferty G, Man W et al (2007) The value of multiple tests of respiratory muscle strength. Thorax 62:975–80
Boussuges A, Gole Y, Blanc P (2009) Diaphragmatic motion studied by m-mode ultrasonography: methods, reproducibility, and normal values. Chest 135:391–400
Cohn D, Benditt JO, Eveloff S, McCool FD (1997) Diaphragm thickening during inspiration. J Appl Physiol 83:291–296
Ueki J, De Bruin PF, Pride NB (1995) In vivo assessment of diaphragm contraction by ultrasound in normal subjects. Thorax 50:1157–1161
Lerolle N, Guerot E, Dimassi S, Zegdi R, Faisy C, Fagon JY et al (2009) Ultrasonographic diagnostic criterion for severe diaphragmatic dysfunction after cardiac surgery. Chest 135:401–407
Kim SH, Na S, Choi JS, Na SH, Shin S, Koh SO (2010) An evaluation of diaphragmatic movement by M-mode sonography as a predictor of pulmonary dysfunction after upper abdominal surgery. Anesthesia Analgesia 110:1349–1354
Matamis D, Soilemezi E, Tsagourias M, Akoumianaki E, Dimassi S, Boroli F et al (2013) Sonographic evaluation of the diaphragm in critically ill patients. Technique and clinical applications. Intensive Care Med 39:801–10
Iverson LI, Mittal A, Dugan DJ, Samson PC (1976) Injuries to the phrenic nerve resulting in diaphragmatic paralysis with special reference to stretch trauma. Am J Surg 132:263–269
Rosett RL (1987) An unusual cause of postoperative respiratory failure. Anesthesiology 66:695–697
Goligher EC, Laghi F, Detsky ME, Farias P, Murray A, Brace D et al (2015) Measuring diaphragm thickness with ultrasound in mechanically ventilated patients: feasibility, reproducibility and validity. Intensive Care Med 41:734
Baldwin CE, Paratz JD, Bersten AD (2011) Diaphragm and peripheral muscle thickness on ultrasound: intra-rater reliability and variability of a methodology using non-standard recumbent positions. Respirology 16:1136–1143
Sarwal A, Parry SM, Berry MJ, Hsu FC, Lewis MT, Justus NW et al. (2015) Interobserver reliability of quantitative muscle sonographic analysis in the critically ill population. J Ultrasound Med Off J Am Instit Ultrasound In Med 34:1191–200
Nava S, Ambrosino N, Crotti P, Fracchia C, Rampulla C (1993) Recruitment of some respiratory muscles during three maximal inspiratory manoeuvres. Thorax 48:702–707
Verin E, Delafosse C, Straus C, Morelot-Panzini C, Avdeev S, Derenne JP et al (2001) Effects of muscle group recruitment on sniff transdiaphragmatic pressure and its components. Eur J Appl Physiol 85:593–598
Vassilakopoulos T, Mastora Z, Katsaounou P, Doukas G, Klimopoulos S, Roussos C et al (2000) Contribution of pain to inspiratory muscle dysfunction after upper abdominal surgery: a randomized controlled trial. American J Respir Crit Care Med 161:1372–1375
Goligher EC, Fan E, Herridge MS, Murray A, Vorona S, Brace D et al (2015) Evolution of diaphragm thickness during mechanical ventilation: impact of inspiratory effort. Am J Respir Crit Care Med 192(9):1080–1088
Evans WJ (2010) Skeletal muscle loss: cachexia, sarcopenia, and inactivity. Am J Clin Nutr 91:1123S–1127S
Laroche CM, Carroll N, Moxham J, Green M (1988) Clinical significance of severe isolated diaphragm weakness. Am Rev Respir Dis 138:862–866
Teitelbaum J, Borel CO, Magder S, Traystman RJ, Hussain SN (1993) Effect of selective diaphragmatic paralysis on the inspiratory motor drive. J Appl Physiol 74:2261–2268
Acknowledgements
The study was funded by FAPESP (Fundação de Amparo e Pesquisa do Estado de Sao Paulo). Grant Number: 2013/11835-6.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Anne Flavia Silva Galindo Santana received a scholarship grant from “Capes” (a non-profit government agency) to participate in the study.All other authors have no conflict of interest with this manuscript.
Research involving human participants and or animals
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Santana, A.F.S.G., Caruso, P., Santana, P.V. et al. Inspiratory muscle weakness, diaphragm immobility and diaphragm atrophy after neck dissection. Eur Arch Otorhinolaryngol 275, 1227–1234 (2018). https://doi.org/10.1007/s00405-018-4923-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-018-4923-6