
Abstract
Purpose
To develop a risk-assessment model for the prediction of emergency cesarean section (CS) in women having induction of labor (IOL).
Methods
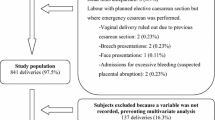
This was an observational cohort study of women with IOL for any indication between 2007 and 2013. Women induced for stillbirths and with multiple pregnancies were excluded. The primary objective was to identify risk factors associated with CS delivery and to construct a risk-prediction tool.
Results
6169 women were identified with mean age of 28.9 years. Primiparity involved 47.1 %, CS rate was 13.3 % and post-date pregnancies were 32.4 %. Risk factors for CS were: age >30 years, BMI >25 kg/m2, primiparity, black-ethnicity, non post-date pregnancy, meconium-stained liquor, epidural analgesia, and male fetal gender. Each factor was assigned a score and with increasing scores the CS rate increased. The CS rate was 5.4 % for a score <11, while for a score ≥11 it increased to 25.0 %. The model had a sensitivity, specificity, negative predictive value and positive predictive value of 75.8, 65.1, 93.8 and 25.0 %, respectively.
Conclusion
We have constructed a risk-prediction tool for CS delivery in women with IOL. The risk-assessment tool for the prediction of emergency CS in induced labor has a high negative-predictive value and can provide reassurance to presumed low-risk women.

Similar content being viewed by others


References
Talaulikar VS, Arulkumaran S (2011) Failed induction of labour: strategies to improve the success rates. Obstet Gynecol Surv 66:717–728
NICE Guideline (2008) Induction of labour. National Collaborating Centre for Women’s and Children’s Health. National Institute for Health and Clinical Excellence. RCOG Press, London
The Information Centre CHS (2006) NHS maternity statistics, England: 2004–2005. The Information Centre, Leeds
National Audit Office (2013) Maternity services in England. Department of Health, HC794. Session 2013–2014
Patterns of Maternity Care in English (2013) NHS Hospitals in 2011/2012. Royal College of Obstetricians and Gynaecologists
Ehrenthal DB, Jiang X, Strobino DM (2010) Labour induction and the risk of a caesarean delivery among nulliparous women at term. Obstet Gynecol 116:35–42
Zhang J, Troendle J, Reddy UM, Laughon SK, Branch DW, Burkman R et al(2010) Contemporary caesarean delivery practice in the United States. Am J Obstet Gynecol 203:326.e1–326.e10
Deneux-Tharaux C, Carmona E, Bouvier-Colle MH, Bréart G (2006) Postpartum maternal mortality and caesarean delivery. Obstet Gynecol 108:541–548
Shorten A (2007) Maternal and neonatal effects of caesarean section. BMJ 335:1003–1004
Yang Q, Wen SW, Oppenheimer L, Chen XK, Black D, Gao J et al (2007) Association of caesarean delivery for first birth with placenta previa and placental abruption in second pregnancy. BJOG 114:609–613
Kaufman KE, Bailit JL, Grobman W (2002) Elective induction an analysis of economic and health consequences. Am J Obstet Gynecol 187:858–863
NICE Clinical Guideline (2011) Costing report caesarean section update. National Institute for Health and Clinical Excellence. RCOG Press, London
Sebire NJ, Jolly M, Harris JP, Wadsworth J, Joffe M, Beard RW et al (2001) Maternal obesity and pregnancy outcome: a study of 287,213 pregnancies in London. Int J Obes Relat Metab Disord 25:1175–1182
Cai QC, Yu ED, Xiao Y, Bai WY, Chen X, He LP et al (2012) Derivation and validation of a prediction rule for estimating advanced colorectal neoplasm risk in average-risk Chinese. Am J Epidemiol 175:584–593
Moons KG, Harrell FE, Steyerberg EW (2002) Should scoring rules be based on odds ratios or regression coefficients? J Clin Epidemiol 55:1054–1055
Steyerberg EW, Bleeker SE, Moll HA, Grobbee DE, Moons KG (2003) Internal and external validation of predictive models: a simulation study of bias and precision in small samples. J Clin Epidemiol 56:441–447
Caughey AB, Sundaram V, Kaimal AJ, Cheng YW, Gienger A, Little SE et al (2009) Maternal and neonatal outcomes of elective induction of labour. Evid Rep Technol Assess (Full Rep) 176:1–257
Rane SM, Guirgis RR, Higgins B, Nicolaides KH (2003) Pre-induction sonographic measurement of cervical length in prolonged pregnancy: the effect of parity in the prediction of the need for caesarean section. Ultrasound Obstet Gynecol 22:45–48
Crane JM (2006) Factors predicting labour induction success: a critical analysis. Clin Obstet Gynecol 49:573–584
Johnson AM, Bellerose L, Billstrom R, Deckers E, Beller P (2014) Evaluating outcomes of labour inductions beyond 39 weeks of gestation. Obstet Gynecol 123(Suppl 1):58S
Boyle A, Reddy UM, Landy HJ, Huang CC, Driggers RW, Laughon SK (2013) Primary caesarean delivery in the United States. Obstet Gynecol 122:33–40
Edmonds JK, Yehezkel R, Liao X, Moore Simas TA (2013) Racial and ethnic differences in primary, unscheduled caesarean deliveries among low-risk primiparous women at an academic medical center: a retrospective cohort study. BMC Pregnancy Childbirth 13:168
Osterman MJ, Martin JA (2013) Changes in caesarean delivery rates by gestational age: United States, 1996–2011. NCHS Data Brief 124:1–8
Smith GC, Cordeaux Y, White IR, Pasupathy D, Missfelder-Lobos H, Pell JP et al (2008) The effect of delaying childbirth on primary caesarean section rates. PLoS Med 5:e144
Torricelli M, Voltolini C, Conti N, Bocchi C, Severi FM, Petraglia F (2013) Weight gain regardless of pre-pregnancy BMI and influence of fetal gender in response to labour induction in postdate pregnancy. J Matern Fetal Neonatal Med 26:1016–1019
Baranova A, Gowder SJ, Schlauch K, Elariny H, Collantes R, Afendy A et al (2006) Gene expression of leptin, resistin, and adiponectin in the white adipose tissue of obese patients with non-alcoholic fatty liver disease and insulin resistance. Obes Surg 16:1118–1125
Bhattacharya S, Campbell DM, Liston WA, Bhattacharya S (2007) Effect of Body Mass Index on pregnancy outcomes in nulliparous women delivering singleton babies. BMC Public Health 7:168
Walker KF, Bugg G, Macpherson M, McCormick C, Wildsmith C, Smith G et al (2012) Induction of labour versus expectant management for nulliparous women over 35 years of age: a multi-centre prospective, randomised controlled trial. BMC Pregnancy Childbirth 12:145
Miller NR, Cypher RL, Foglia LM, Pates JA, Nielsen PE (2014) Elective induction of nulliparous labour at 39 weeks of gestation: a randomized clinical trial. Obstet Gynecol 123(Suppl 1):72S
Lee KA, Mi Lee S, Jin Yang H, Park CW, Mazaki-Tovi S, Hyun Yoon B et al (2011) The frequency of meconium-stained amniotic fluid increases as a function of the duration of labour. J Matern Fetal Neonatal Med 24:880–885
Becker S, Solomayer E, Dogan C, Wallwiener D, Fehm T (2007) Meconium-stained amniotic fluid–perinatal outcome and obstetrical management in a low-risk suburban population. Eur J Obstet Gynecol Reprod Biol 132:46–50
NICE Guideline (2004) Caesarean section. National Collaborating Centre for Women’s and Children’s Health. National Institute for Health and Clinical Excellence. RCOG Press, London
Torricelli M, Voltolini C, Vellucci FL, Conti N, Bocchi C, Severi FM et al (2013) Fetal gender effects on induction of labour in postdate pregnancies. Reprod Sci 20:670–674
Buckberry S, Bianco-Miotto T, Bent SJ, Dekker GA, Roberts CT (2014) Integrative transcriptome meta-analysis reveals widespread sex-biased gene expression at the human fetal-maternal interface. Mol Hum Reprod 20:810–819
Misra DP, Salafia CM, Miller RK, Charles AK (2009) Non-linear and gender-specific relationships among placental growth measures and the fetoplacental weight ratio. Placenta 30:1052–1057
Agarwal U, Anastasakis E, Kadir RA (2009) The effect of fetal sex on the outcome of labour induction. J Obstet Gynaecol 29:711–713
Eogan MA, Geary MP, O’Connell MP, Keane DP (2003) Effect of fetal sex on labour and delivery: retrospective review. BMJ 326:137
Grobman WA (2012) Predictors of induction success. Semin Perinatol 36:344–347
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
None.
Conflict of interest
The authors declare that they have no conflict of interest.
Research involving human participants and/or animals
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Our study was a retrospective study, and for this type of study formal consent is not required.
Rights and permissions
About this article

Cite this article
Papoutsis, D., Antonakou, A., Gornall, A. et al. The SaTH risk-assessment tool for the prediction of emergency cesarean section in women having induction of labor for all indications: a large-cohort based study. Arch Gynecol Obstet 295, 59–66 (2017). https://doi.org/10.1007/s00404-016-4209-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-016-4209-4