
Summary
The individual adjustment of the AV intervals is a prerequisite for the hemodynamic advantages of dual-chamber pacing. The methods for the optimization of the AV delay (AVD), applied so far, are time intensive. A simple and fast method is the approximate adjustment of the AVD with the surface- and vector-ECG. The optimal AVD is obtained if at the end of the atrial contraction the mitral valve is closed by the ventricular increase of pressure. In order to achieve this with pacemaker patients, the individually different atrial and ventricular conduction times must be considered. The different conduction times can be determined from surface- and vector-ECG. Intra- and interatrial conduction times can be defined by the beginning of the atrial spike up to the end of the p-wave. The begin of ventricular pressure increase corresponds to the peak of the stimulated QRS complex (beginning of the iso-volumetric contraction time, ISVC) and depends on the interventricular conduction time.
With 100 patients, who did not receive a cardiac pacemaker, the interval at the end of the p-wave (left atrial excitation, EP) up to the peak of the R-wave (ISVC) during rest and exercise was measured and an age-referred average value of 100 ms was determined; this serves as a standard value, if no AV conduction is available. The approximated optimized AVD is used if the interval of the end at the p-wave to the peak of the QRS complex is equal to 100 ms. Over a simple algorithm, the optimized AVD can be calculated as follows:
After programming a long AVD, the interval at the end of the native or paced p-wave up to the peak of the stimulated QRS complex (EP/ISVC) is determined. The EP/ISVC value found is taken from the long AVD, the 100ms standard value now is added and one receives the approximated optimized AVD.
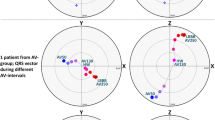
It is not always easy to determine the end of the p-wave from the surface ECG, especially for the paced atrium. Therefore, with a special computer program we can create a vector-cardiogram from the 12 lead-ECG. The endpoint of the p-wave vector loop corresponds with the end of atrial excitation.
For validating the described method, 13 consecutive patients (2 female, 11 male, average age 67 ± 7.8 years) were included, and received for different indications (7 sick sinus syndrome, 4 AV block III, 2 binode disease) a DDD pacemaker (Affinity, St. Jude Medical).
About 8 weeks after implantation all patients underwent a PA catheter investigation, in order to optimize the AV-/PV delay of the pacemaker regarding the maximum cardiac output (CO). For CO measurement the thermodilution method was applied. Altogether 17 complete hemodynamic measurements (9 times with different PVDs, 8 times with different AVDs) were executed. Patients No. 10 to 13 could be examined both in the VDD and in the DDD mode.
The minimum determined CO amounted to 3.5 l/min, the maximal CO 7.1 l/min and the average value 5.62 ± 0.98 l/min. No optimal AVD was found in any of the patients. A different broad interval of AVDs with optimal CO results were obtained. The comparison of the surface ECG optimized AVD with the PA catheter optimized AVD showed a statistically significant correlation (0.825PV, 0.982 AV, P < 0.01). Sixteen out of seventeen measurements were at an interval which enables hemodynamic optimal CO or stroke volume. Only one AVD determined from the surface ECG was situated slightly (10 ms) outside of the hemodynamically optimally determined AVD.
Zusammenfassung
Die bisher angewandten Methoden zur Optimierung der AV-Zeiten bei 2-Kammerschrittmacher erfordern einen gewissen apparativen Aufwand und sind zeitintensiv. Eine einfache und schnelle Methode ist die approximative Einstellung der AV-Intervalle mit Hilfe des Ober.ächen- und des Vektor-EKGs.
Das optimale AV-Intervall (AVI) ist dann gegeben, wenn am Ende der atrialen Kontraktion die Mitralklappe durch den ventrikulären Druckanstieg geschlossen wird. Bei Schrittmacherpatienten müssen die individuell unterschiedlichen atrialen und ventrikulären elektrophysiologischen Leitungszeiten berücksichtigt werden. Mit Hilfe des Oberflächen- und Vektor-EKGs lassen sich die unterschiedlichen Leitungszeiten feststellen. Die atriale Leitungszeit wird vom Beginn des atrialen Stimulus bis zum Ende der P-Welle definiert. Die Spitze des stimulierten Kammerkomplexes im EKG ist abhängig von der interventrikulären Leitungszeit. Der ventrikuläre Druckanstieg korrespondiert mit der Spitze des stimulierten Kammerkomplexes (Beginn der isovolumetrischen Kontraktionszeit, ISVK). Bei 100 Patienten, die keinen Herzschrittmacher tragen, wurde das Intervall vom Ende der P-Welle (linksatriale Erregung, EP) bis zum Gipfel der R-Welle (ISVK) in Ruhe und unter Belastung gemessen und ein altersbezogener Mittelwert von 100 ms festgestellt, dieser dient als Referenzwert für die Einstellung der AVI. Die approximierte optimierte AV-Zeit ist dann gegeben, wenn das Intervall vom Ende der P-Welle (linksatriale Erregung) bis zur Spitze des stimulierten Kammerkomplexes 100 ms beträgt. Über einen einfachen Algorithmus wird das approximativ optimierte AV-Intervall berechnet.
Ein bewusst langes AVI wird eingestellt und das Intervall vom Ende der nativen oder stimulierten P-Welle bis zur Spitze des stimulierten Kammerkomplexes (EP/ISVK) bestimmt. Der gefundene Wert EP/ISVK wird nun vom langen AVI abgezogen, als Referenzwert werden nun 100 ms addiert, und man erhält das approximativ optimierte AVI.
Das Ende der P-Welle ist aus dem Oberflächen-EKG nicht immer einfach zu bestimmen, dies trifft besonders für den stimulierten Vorhof zu. Über ein spezielles Computerprogramm (SEMA, Fa. Schiller), lässt sich aus einem digitalen EKG mit 12 Ableitungen ein Vektorkardiogramm für die P-Welle erstellen, wobei der Endpunkt der Vektorschleife das Ende der atrialen Erregung definiert. Mit der Cursor-Funktion kann die Zeit EP/ISVK einfach bestimmt werden.
Zur Validierung der beschriebenen Methode wurden 13 konsekutive Patienten (2 Frauen, 11 Männer, Durchschnittsalter: 67 ± 7,8 Jahre) eingeschlossen, die aus unterschiedlicher Indikation (7-mal Sick-sinus-Syndrom, 4-mal AV Block Grad 3, 2-mal 2-Knotenkrankheit) einen DDD-Schrittmacher (Affinity, St. Jude Medical) erhielten. Etwa 8 Wochen nach der Implantation unterzogen sich alle Patienten einer PA-Katheter-Untersuchung, um die AV-/PV-Zeiten des Schrittmachers im Hinblick auf das zu erzielende maximale Herzzeitvolumen (HZV) zu optimieren. Zur HZV-Messung wurde das Thermodilutionsprinzip angewandt.
Insgesamt wurden 17 vollständige hämodynamische Messungen (9-mal mit verschiedenen PV-, 8-mal mit verschiedenen AV-Zeiten) durchgeführt. Die Patienten Nr. 10–13 konnten sowohl im VDD- als auch im DDD-Modus untersucht werden.
Das minimal bestimmte optimale HZV betrug 3,5 l/min.; das maximale 7,1 l/min., und der Mittelwert betrug 5,62 ± 0,98 l/min. Bei allen Patienten fand sich dabei nicht nur eine einzige optimale AV-/PV-Zeit, sondern ein unterschiedlich breites Intervall von nebeneinander liegenden AV-/PV-Zeiten, bei denen jeweils optimale HZV-Ergebnisse zu erzielen waren.
Der Vergleich der vom Oberflächen EKG ermittelten optimierten AV-/PV-Werte mit den hämodynamisch gemessenen optimierten AV-/PV-Intervallen zeigte eine statistisch signifikante Korrelation (0,825PVI, 0,982 AVI, p < 0,01). Insgesamt 16 von 17 Messungen liegen in einem Intervall, das hämodynamisch optimale HZV bzw. Schlagvolumina ermöglicht, nur einmal lag ein vom Oberflächen EKG ermittelter PV-Wert geringfügig (10 ms) außerhalb des als hämodynamisch optimal bestimmten Intervalls.
Similar content being viewed by others


Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Koglek, W., Kranig, W., Kowalski, M. et al. Eine einfache Methode zur Bestimmung des AV-Intervalls bei 2-Kammerschrittmachern. Herzschr Elektrophys 15 (Suppl 1), i23–i32 (2004). https://doi.org/10.1007/s00399-004-1104-7
Issue Date:
DOI: https://doi.org/10.1007/s00399-004-1104-7