
Abstract
Background
ACCORD and SPRINT are the best randomized controlled trial data evaluating the effects of blood pressure targets below 140 mmHg. These trials had contradictory results regarding the benefits of intensive antihypertensive therapy. We investigate if this discordance was driven by SPRINT’s inclusion of Heart Failure in its primary outcome, as this is a parameter not included in ACCORD’s original primary outcome. This analysis helps to resolve a significant area of contention.
Methods
Individual patient data from 4733 participants in ACCORD were analyzed from time of randomization. All participants were diabetic and at increased cardiovascular risk. Participants were assigned to their original intervention, a standard blood pressure target of less than 140 mmHg or an intensive target of less than 120 mmHg. Primary composite outcome was defined as in SPRINT: a composite of first occurrence of myocardial infarction, stroke, heart failure, death from cardiovascular causes, and other acute coronary syndromes.
Results
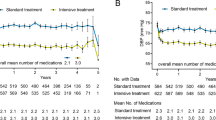
Primary outcome was not significantly different between standard and intensive groups [HR: 0.89; 95% CI: (0.76–1.03); p = 0.108]. The primary composite outcome occurred in 370 participants in the standard group (15.6%) and 324 participants in the intensive group (13.7%), with an event rate of 3.38% per year for the standard group and 3.01% per year for the intensive group.
Conclusions
Differing results between ACCORD and SPRINT are not attributable to ACCORD’s exclusion of Heart Failure from its original primary outcome measurement. No significant differences in primary outcome were observed between intensive and standard blood pressure groups in the ACCORD patients under the SPRINT primary outcome definition. Caution should be taken in extrapolating the intensive blood pressure control benefits of SPRINT to the diabetic population.

Similar content being viewed by others


References
Smulders YM, Muller M (2016) Blood pressure lowering for cardiovascular disease. Lancet 388:125–126
Vidal-Petiot E, Ford I, Greenlaw N et al (2016) Cardiovascular event rates and mortality according to achieved systolic and diastolic blood pressure in patients with stable coronary artery disease: an international cohort study. Lancet 388:2142–2152
Tobe SW, Izzo JL Jr (2016) Controversies in hypertension: is lower blood pressure always better? J Am Soc Hypertens 10:618–620
Mahfoud F, Schmieder RE, Azizi M et al (2017) Proceedings from the 2nd European Clinical Consensus conference for device-based therapies for hypertension: state of the art and considerations for the future. Eur Heart J 38:3272–3281
Sarafidis PA, Lazaridis AA, Ruiz-Hurtado G, Ruilope LM (2017) Blood pressure reduction in diabetes: lessons from ACCORD, SPRINT and EMPA-REG OUTCOME. Nat Rev Endocrinol 13:365–374
Filippone EJ, Foy AJ (2016) Blood pressure management in the wake of SPRINT. Cleve Clin J Med 83:196–198
Krakoff LR (2016) A Tale of 3 Trials: ACCORD, SPRINT, and SPS3. What Happened? Am J Hypertens 29:1020–1023
ACCORD Study Group, Cushman WC, Evans GW, et al (2010) Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med 362:1575–1585
SPRINT Research Group, Wright JT Jr, Williamson JD, et al (2015) A randomized trial of intensive versus standard blood-pressure control. N Engl J Med 373:2103–2116
Weiss J, Freeman M, Low A et al (2017) Benefits and harms of intensive blood pressure treatment in adults aged 60 years or older: a systematic review and meta-analysis. Ann Intern Med 166:419–429
Cushman WC, Whelton PK, Fine LJ et al (2015) SPRINT trial results. Hypertension HYPERTENSIONAHA.115.06722
Perkovic V, Rodgers A (2015) Redefining blood-pressure targets—SPRINT starts the marathon. N Engl J Med 373:2175–2178
Mancia G The SPRINT trial: Cons. In: American College of Cardiology—Latest in Cardiology. Accessed 2 Dec 2015
Thomopoulos C, Parati G, Zanchetti A (2016) Effects of blood pressure lowering on outcome incidence in hypertension. J Hypertens 34:613–622
Tschöpe C, Birner C, Böhm M et al (2018) Heart failure with preserved ejection fraction: current management and future strategies: expert opinion on the behalf of the Nucleus of the “Heart Failure Working Group” of the German Society of Cardiology (DKG). Clin Res Cardiol 107:1–19
Legrand M, Ludes P-O, Massy Z et al (2017) Association between hypo- and hyperkalemia and outcome in acute heart failure patients: the role of medications. Clin Res Cardiol. https://doi.org/10.1007/s00392-017-1173-3
Bistola V, Simitsis P, Farmakis D et al (2018) Association of mineralocorticoid receptor antagonist use and in-hospital outcomes in patients with acute heart failure. Clin Res Cardiol 107:76–86
Weir MR, Bakris GL (2010) Optimal blood pressure for a patient with type 2 diabetes mellitus: insight from the ACCORD study. Curr Hypertens Rep 12:313–315
Acknowledgements
SPRINT and ACCORD trialist groups for their significant efforts in conducting the clinical trials. National Heart, Lung, and Blood Institute, BioLINCC data repository for storing and providing access to the ACCORD and SPRINT datasets. The opinions and views presented in this manuscript do not necessarily reflect those of SPRINT, ACCORD, or BioLINCC (NHLBI).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Rights and permissions
About this article

Cite this article
Aggarwal, R., Mirzan, H., Chiu, N. et al. Heart failure and the discrepancy between trials of intensive blood pressure management: an analysis of individual patient data. Clin Res Cardiol 107, 565–569 (2018). https://doi.org/10.1007/s00392-018-1218-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-018-1218-2