
Abstract
Purpose
Patients with a chronic comorbidity or multiple comorbidities are at much greater risk of serious colonoscopy-related gastrointestinal (GI) adverse events relative to patients with no comorbidity. It is important to identify outpatient facilities that can effectively and safely provide colonoscopy to complex patients. To address this need, the association between outpatient facilities’ complex care volume and type (ambulatory surgery center (ASC) and hospital outpatient department (HOPD)) and the risks of serious GI adverse events in colonoscopy patients with single and multiple chronic comorbidities were examined.
Methods
Outpatient colonoscopies of 1,020,372 patients with single and multiple comorbidities were investigated, using a retrospective cohort study. Thirty-day hospitalizations due to colonic perforations and GI bleeding were examined. Ambulatory surgery and hospital discharge datasets from California, Florida, and New York for 2006–2009 were used.
Results
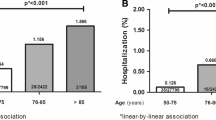
Higher complex care volume was associated with lower risks of adverse events in patients with comorbidities (OR 1.69; 95% CI [1.13, 2.54]). ASCs had higher risks of adverse events in patients with comorbidities relative to HOPDs (OR 2.85; 95% CI [2.40, 3.38]). Patients with single and multiple comorbid conditions, patients with systemic diseases, and complex patients of advanced age had higher risks of adverse events.
Conclusions
Referring patients with single and multiple chronic comorbidities to facilities experienced in treating complex patients, or HOPDs, may reduce colonoscopy-related adverse events.

Similar content being viewed by others


References
American Cancer Society (ACS) (2018) Cancer facts & figures. Retrieved August 2018, from https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2018/cancer-facts-and-figures-2018.pdf
Zauber AG, Winawer SJ, O'Brien MJ, Lansdorp-Vogelaar I, van Ballegooijen M, Hankey BF, Shi W, Bond JH, Schapiro M, Panish JF, Stewart ET, Waye JD (2012) Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N Engl J Med 366(8):687–696
Center for Disease Control and Prevention (CDC) (2016) Colorectal cancer screening capacity in the U.S. Retrieved August 2018, from https://www.cdc.gov/cancer/dcpc/research/articles/crc_screening_model.htm
Chukmaitov A, Siangphoe U, Dahman B, Bradley CJ, BouHaidar D (2016) Patient comorbidity and serious adverse events after outpatient colonoscopy: population-based study from three states, 2006 to 2009. Dis Colon Rectum 59(7):677–687
Rabeneck L, Paszat LF, Hilsden RJ, Saskin R, Leddin D, Grunfeld E, Wai E, Goldwasser M, Sutradhar R, Stukel TA (2008) Bleeding and perforation after outpatient colonoscopy and their risk factors in usual clinical practice. Gastroenterology. 135(6):1899–1906
Chowdhury MM, Dagash H, Pierro A (2007) A systematic review of the impact of volume of surgery and specialization on patient outcome. Br J Surg 94(5):145–161
Chukmaitov AS, Menachemi N, Brown SL, Saunders C, Tang A, Brooks R (2008a) Is there a relationship between physician and facility volumes of ambulatory procedures and patient outcomes? J Ambul Care Manage 31(4):354–369
Chukmaitov AS, Menachemi N, Brown LS, Saunders C, Brooks RG (2008b) A comparative study of quality outcomes in freestanding ambulatory surgery centers and hospital-based outpatient departments: 1997-2004. Health Serv Res 43(5 Pt 1):1485–1504
Fleisher LA, Pasternak LR, Herbert R, Anderson GF (2004) Inpatient hospital admission and death after outpatient surgery in elderly patients: importance of patient and system characteristics and location of care. Arch Surg 139(1):67–72
Ranasinghe I, Parzynski CS, Searfoss R, Montague J, Lin Z, Allen J, Vender R, Bhat K, Ross JS, Bernheim S, Krumholz HM, Drye EE (2016) Differences in colonoscopy quality among facilities: development of a post-colonoscopy risk-standardized rate of unplanned hospital visits. Gastroenterology. 150(1):103–113
Winter A (2003) Comparing the mix of patients in various outpatient surgery settings. Health Aff 22(6):68–75
Ko CW, Dominitz JA (2010) Adverse events of colonoscopy: magnitude and management. Gastrointest Endosc Clin N Am 20:659–671
Chukmaitov A, Bradley CJ, Dahman B, Siangphoe U, Warren JL, Klabunde CN (2013) Association of polypectomy techniques, endoscopist volume, and facility type with colonoscopy complications. Gastrointest Endosc 77(3):436–446
Elixhauser A, Steiner C, Harris DR, Coffey RM (1998) Comorbidity measures for use with administrative data. Med Care 36(1):8–27
Menachemi N, Chukmaitov A, Brown LS, Saunders C, Brooks RG (2007) Quality of care differs by patient characteristics: outcome disparities after ambulatory surgical procedures. Am J Med Qual 22(6):395–401
Firth D (1993) Bias reduction of maximum likelihood estimates. Biometrika 80:27–38
Watabe H, Yamaji Y, Okamoto M, Kondo S, Ohta M, Ikenoue T, Kato J, Togo G, Matsumura M, Yoshida H, Kawabe T, Omata M (2006) Risk assessment for delayed hemorrhagic complication of colonic polypectomy: polyp-related factors and patient-related factors. Gastrointest Endosc 64(1):73–78
Hui AJ, Wong RM, Ching JY, Hung LC, Chung SC, Sung JJ (2004) Risk of colonoscopic polypectomy bleeding with anticoagulants and antiplatelet agents: analysis of 1657 cases. Gastrointest Endosc 59(1):44–48
Lee JW (2010) Fluid and electrolyte disturbances in critically ill patients. Electrolyte Blood Press 8(2):72–81
Centers for Medicare and Medicaid Services (CMS) (2015) CMS proposes hospital outpatient and ambulatory surgical center policy and payment changes, including proposed changes to the two-midnight rule, and quality reporting changes for 2016. Retrieved in June 2018, from https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2015-Fact-sheets-items/2015-07-01.html
Medicare Payment Advisory Commission (MedPAC) (2017) Report to the congress: Medicare payment policy. Ambulatory surgical center services. Retrieved in June 2018, from http://www.medpac.gov/docs/default-source/reports/mar17_entirereport.pdf
Funding
The VCU Massey Cancer Center pilot grant (CA016059) was used to purchase the Healthcare Cost and Utilization Project’s (HCUP) datasets for this study. Services in support of the research project were generated by the VCU Massey Cancer Center Biostatistics Shared Resource, supported, in part, with funding from NIH-NCI Cancer Center Support Grant P30 CA016059.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chukmaitov, A., Dahman, B. & Bradley, C.J. Outpatient facility volume, facility type, and the risk of serious colonoscopy-related adverse events in patients with comorbid conditions: a population-based study. Int J Colorectal Dis 34, 1203–1210 (2019). https://doi.org/10.1007/s00384-019-03304-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-019-03304-3