
Abstract
Purpose
In Western medical centers, emphasis has been placed on simultaneous myelomeningocele closure and ventriculoperitoneal shunting for children with spina bifida (SB) and co-morbid hydrocephalus (HC). This is not practical in developing countries where patients present in a delayed fashion, many with open, dirty myelomeningoceles. The purpose of this study was to evaluate whether timing of shunting in relation to myelomeningocele closure affected shunt-related complications such as SB wound infection, shunt infection, and shunt malfunction.
Methods
A retrospective analysis was undertaken of all SB patients undergoing ventriculoperitoneal shunting within 11 days following myelomeningocele closure at Kijabe Hospital between 1997 and August 2007. Data were collected from hospital records and analyzed in SPSS.
Results
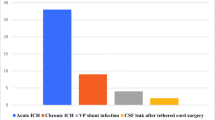
Over the study period there were 276 patients included. Eighteen patients were shunted prior to SB closure and 13 patients had simultaneous shunting and SB closure. Patients shunted prior to, simultaneously, or within the first 4 days after SB closure had a fivefold higher shunt infection rate (23%) than those shunted 5–10 days following SB closure (4.7%) (p < 0.0001). Shunt malfunctions were also significantly higher in the group shunted prior to back closure (33.3%) vs. those shunted simultaneously (15.4%) or within the first 10 days following SB closure (13.9%) (p = 0.0001). No difference was seen in these groups with regard to wound infections. No difference in shunt-related complications was observed between those shunted 5 to 10 days following back closure.
Conclusions
This study indicates that in developing countries, patients with SB who present in a delayed fashion but require shunting and have sterile CSF, should have their shunts inserted 5–10 days after SB closure.




Similar content being viewed by others

References
Yen IH, Khoury MJ, Erickson JD et al (1992) The changing epidemiology of neural tube defects. Am J Dis Child 146:857–861
Park TS (1999) Myelomeningocele. In: Albright AL, Pollack IF, Adelson PD (eds) Principles and practice of pediatric neurosurgery. Thieme Medical Publishers, Inc., New York, pp 291–320
Stevenson RE, Allen WP, Pai GS, Best R, Seaver LH, Dean J, Thompson S (2000) Decline in prevalence of neural tube defects in a high-risk region of the United States. Pediatrics 106(4):825–827
Zheng XY, Song XM, Chen G, Chen JP, Ji Y, Wu JL, Liu JF, Zhang L, Fan XH (2007) Epidemiology of birth defects in high-prevalence areas of China. Zhonghua Liu Xing Bing Xue Za Zhi 28(1):5–9
Li Z, Ren A, Zhang L, Ye R, Li S, Zheng J, Hong S, Wang T, Li Z (2006) Extremely high prevalence of neural tube defects in a 4-county area in Shanxi Province, China. Birth Defects Res A Clin Mol Teratol 76(4):234–240
MRC Vitamin Study Research Group (1991) Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. Lancet 338:131–137
Czeizel AE, Dudas I (1992) Prevention of the first occurrence of neural tube defects by periconceptional vitamin supplementation. N Engl J Med 327:1832–1835
Roberts HE, Moore CA, Cragan JD et al (1995) Impact of prenatal diagnosis on the birth prevalence of neural tube defects, Atlanta, 1990–91. Pediatrics 96:880–883
Steinbok P, Irvine B, Cochrane DD, Irwin BJ (1992) Long-term outcome and complications of children born with meningomyelocele. Childs Nerv Syst 8(2):92–96
Stein SC, Schut L (1979) Hydrocephalus in myelomeningocele. Child’s Brain 5:413–419
Bowman RM, McLone DG, Grant JA, Tomita T, Ito JA (2001) Spina bifida outcome: a 25-year prospective. Pediatr Neurosurg 34(3):114–120
DiRocco C, Massimi L, Tamburrini G (2006) Shunts vs endoscopic third ventriculostomy in infants: are there different types and/or rates of complications? A review. Childs Nervous Syst 22:1573–1589
Ribaupierre S, Rilliet B, Vernet O, Regli L, Villemure JG (2007) Third ventriculostomy vs ventriculoperitoneal shunt in pediatric obstructive hydrocephalus: results from a Swiss series and literature review. Childs Nerv Syst 23:527–533
Marlin AE (2004) Management of hydrocephalus in the patient with myelomeningocele: an argument against third ventriculostomy. Neurosurg Focus 15(2):1–3
Beems T, Grotenhuis JA (2002) Is the success rate of endoscopic third ventriculostomy age-dependent? An analysis of the results of endoscopic third ventriculostomy in young children. Childs Nerv Syst 18:605–608
Warf BC. Hydrocephalus in Uganda: the predominance of infectious origin and primary management with endoscopic third ventriculostomy. J Neurosurg 1021–1015
Caldarelli M, Di Rocco C, LaMarca F (1996) Shunt complications in the first postoperative year in children with meningomyelocele. Childs Nerv Syst 12(12):478–454
Mwang’ombe NJ, Omulo T (2000) Ventriculoperitoneal shunt surgery and shunt infections in children with non-tumour hydrocephalus at the Kenyatta National Hospital, Nairobi. East Afr Med J 77(7):386–390
Kulkarni AV, Drake JM, Lamberti-Pasculli M (2001) Cerebrospinal fluid shunt infection: a prospective study of risk factors. J Neurosurg 94(2):195–201
Odio C, McCracken GH Jr, Nelson JD (1984) CSF shunt infections in pediatrics. A seven-year experience. Am J Dis Child 138(12):1103–1108
Morissette I, Gourdeau M, Francoeur J (1993) CSF shunt infections: a fifteen-year experience with emphasis on management and outcome. Can J Neurol Sci 20(2):118–122
Ammirati M, Raimondi AJ (1987) Cerebrospinal fluid shunt infections in children. A study on the relationship between the etiology of hydrocephalus, age at the time of shunt placement and infection rate. Childs Nerv Syst 3(2):106–109
Choux M, Genitori L, Lang D, Lena G (1992) Shunt implantation: reducing the incidence of shunt infection. J Neurosurg 77(6):875–880
Kontny U, Hofling B, Gutjahr P, Voth D, Schwarz M, Schmitt HJ (1993) CSF shunt infections in children. Infection 21(2):89–92
George R, Leibrock L, Epstein M (1979) Long term analysis of cerebrospinal fluid shunt infections. A 25 year experience. J Neurosurg 51:804–811
Borgbjerg BM, Gjerris F, Albeck MJ, Borgesen SE (1995) Risk of infection after cerebrospinal fluid shunt: an analysis of 884 first-time shunts. Acta Neurochirurgica 136(1–2):1–7
Rotim K, Miklic P, Paladino J, Melada A, Marcikic M, Scap M (1997) Reducing the incidence of infection in pediatric cerebrospinal fluid shunt operations. Childs Nerv Syst 13:584–587
Quigley MR, Reigel DH, Kortyna R (1989) Cerebrospinal fluid shunt infections. Report of 41 cases and critical review of the literature. Pediatr Neurosci 15(3):111–120
Epstein NE, Rosenthal AD, Zito J, Osipoff M (1985) Shunt placement and myelomeningocele repair: simultaneous vs. sequential shunting. Review of 12 cases. Childs Nerv Syst 1(3):145–147
Parent AD, McMillan T (1995) Contemporaneous shunting with repair of myelomeningocele. Pediatr Neursurg 22(3):132–135
Machado HR, Santos De Oliveira R (2004) Simultaneous repair of myelomeningocele and shunt insertion. Childs Nerv Syst 20(2):107–109
Albright AL, Pollack IF, Adelson PD (2001) Operative techniques in pediatric neurosurgery. Thieme Medical Publishers, Inc, New York, pp 3–14, 75–88
Kallen B, Cocchi G, Knudsen LB et al (1994) International study of sex ratio and twinning of neural tube defects. Teratology 50:322–331
Acknowledgment
International Federation for Spina Bifida and Hydrocephalus (IFSBH).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Margaron, F.C., Poenaru, D., Bransford, R. et al. Timing of ventriculoperitoneal shunt insertion following spina bifida closure in Kenya. Childs Nerv Syst 26, 1523–1528 (2010). https://doi.org/10.1007/s00381-010-1156-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-010-1156-4