
Abstract
Objective
To describe the incidence, predisposing factors and management of postoperative vesicoureteral reflux (VUR) after high-pressure balloon dilation to treat primary obstructive megaureter (POM).
Materials and methods
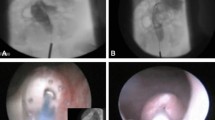
We have reviewed patients that underwent endoscopic treatment for POM from May 2008 to November 2013. All patients were evaluated with renal ultrasound, voiding cystourethrography and diuretic renogram. Endoscopic treatment was done with high-pressure balloon dilation of the ureterovesical junction under general anesthesia; a double-J stenting was done in all patients. Follow-up was performed with ultrasonography, voiding cystourethrography and a diuretic renogram in all patients.
Results
Fifteen boys and five girls with a mean age of 14.18 months (3–103) were reviewed. A total of 22 ureters underwent HPBD to treat POM. Ureterohydronephrosis improves in 19 ureters. After endoscopic treatment, six ureters developed VUR. Four ureters were managed surgically, and in the other two, VUR disappeared in a second cystogram. The presence of parameatal diverticulum in the preoperative cystography and those patients with bilateral POM are factors related to postoperative VUR (p < 0.05). Urinary tract infection after HPBD was observed in four patients, but only one of them was affected with VUR.



Similar content being viewed by others


References
DeFoor W, Minevich E, Reddy P, Polsky E, McGregor A, Wacksman J et al (2004) Results of tapered ureteral reimplantation for primary megaureter: extravesical versus intravesical approach. J Urol 172:1640–1643
Angulo JM, Arteaga R, Rodrıguez Alarcon J, Calvo MJ (1998) Role of retrograde endoscopic dilatation with balloon and derivation using double pig-tail catheter as an initial treatment for vesicoureteral junction stenosis in children. Cir Pediatr 11:15–18
Capozza N, Torino G, Nappo S, Collura G, Mele E (2015) Primary obstructive megaureter in infants: our experience with endoscopic balloon dilation and cutting balloon ureterotomy. J Endourol 29(1):1–5
Kajbafzadeh AM, Payabvash S, Salmasi AH, Arshadi H, Hashemi SM, Arabian S (2007) Endoureterotomy for treatment of primary obstructive megaureter in children. J Endourol 21:743–749
Romero RM, Angulo JM, Parente A, Rivas S, Tardaguila AR (2014) Primary obstructive megaureter: the role of high pressure balloon dilation. J Endourol 28:517–523
García-Aparicio L, Rodo J, Krauel L, Palazon P, Martin O, Ribó JM (2012) High pressure balloon dilation of the ureterovesical junction-first line approach to treat primary obstructive megaureter? J Urol 187:1834–1838
Angerri O, Caffaratti J, Garat JM, Villavicencio H (2007) Primary obstructive megaureter initial experience with endoscopic dilatation. J Endourol 21:999–1004
Christman MS, Kasturi S, Lambert SM, Kovell RC, Casale P (2012) Endoscopic management and the role of double stenting for primary obstructive megaureters. J Urol 187:1018–1022
Garcia-Aparicio L, Blazquez-Gomez E, Martin O, Palazon P, Manzanares A, García-Smith N et al (2013) Use of high-pressure balloon dilatation of the ureterovesical junction instead of ureteral reimplantation to treat primary obstructive megaureter: is it justified? J Pediatr Urol 9(6):1229–1233
Conflicts of interest
All the authors declare no conflicts of interest.
Ethical standard
All patients have signed informed consent prior to this study. Our ethical board committee has accepted this clinical study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
García-Aparicio, L., Blázquez-Gómez, E., de Haro, I. et al. Postoperative vesicoureteral reflux after high-pressure balloon dilation of the ureterovesical junction in primary obstructive megaureter. Incidence, management and predisposing factors. World J Urol 33, 2103–2106 (2015). https://doi.org/10.1007/s00345-015-1565-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-015-1565-9