
Abstract
Purpose
To validate a split-bolus contrast injection protocol for single-phase CBCT in terms of detectability of hypovascular liver tumors compared to digital subtraction angiography (DSA).
Materials and Methods
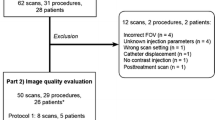
In this retrospective, single-center study, 20 consecutive patients with in total 77 hypovascularized tumors referred for intra-arterial therapy received a split-bolus single-phase CBCT. Two readers rated the visibility of the target tumors scheduled for embolization in CBCT and DSA compared to the pre-interventional multiphasic CT or MRI used as reference on a 3-point scoring system (1 = optimal, 3 = not visible) and catheter-associated artifacts (1 = none, 3 = extended). SNR, CNR and contrast values were derived from 37 target tumors in CBCT and MRI. Statistical analysis included the kappa test to determine interrater reliability, the Friedman’s test for the inter-modality comparison evaluating tumor visibility in DSA and CBCT as well as for quantitative assessment. Post hoc analysis included the Wilcoxon signed-rank test. p values < 0.05 were considered significant.
Results
Ninety percentage of target tumors were rated as visible in CBCT and 37.5% in DSA (p < 0.001). 70.1% of pre-interventionally detected hypovascularized tumors were depicted with CBCT and 31.2% by DSA (p < 0.001). 7.8% of known tumors were outside the FOV. Quantitative assessment showed higher image contrasts in CBCT (1.91 ± 7.01) compared to hepatobiliary-phase MRI (0.29 ± 0.14, p = 0.003) and to portal-venous (p.v.) MRI (0.31 ± 0.13, p < 0.001), but higher CNR for MRI (1.18 ± 0.80; 13.92 ± 15.82; 13.79 ± 6.65).
Conclusion
In conclusion, the split-bolus single-phase CBCT detects significantly more hypovascularized liver tumors compared to DSA performed through the proper hepatic artery with high image contrasts.
Level of Evidence
Level III, diagnostic study.


Similar content being viewed by others
References
Zech CJ, Herrmann KA, Reiser MF, Schoenberg SO. MR imaging in patients with suspected liver metastases: value of liver-specific contrast agent Gd-EOB-DTPA. Magn Reson Med Sci Off J Jpn Soc Magn Res Med. 2007;6:43–52.
Fernandez R, Pappas SG, Bentrem DJ. Clinical features of metastatic hepatic malignancies. Cancer Treat Res. 2016;168:185–202.
Schernthaner RE, Haroun RR, Duran R, et al. Improved visibility of metastatic disease in the liver during intra-arterial therapy using delayed arterial phase cone-beam CT. Cardiovasc Intervent Radiol. 2016;39:1429–37.
Reimer P, Rummeny EJ, Daldrup HE, et al. Enhancement characteristics of liver metastases, hepatocellular carcinomas, and hemangiomas with Gd-EOB-DTPA: preliminary results with dynamic MR imaging. Eur Radiol. 1997;7:275–80.
Zech CJ, Korpraphong P, Huppertz A, et al. Randomized multicentre trial of gadoxetic acid-enhanced MRI versus conventional MRI or CT in the staging of colorectal cancer liver metastases. Br J Surg. 2014;101:613–21.
Namasivayam S, Martin DR, Saini S. Imaging of liver metastases: mRI. Cancer Imaging. 2007;7:2–9.
Padia SA, Lewandowski RJ, Johnson GE, et al. Radioembolization of hepatic malignancies: background, quality improvement guidelines, and future directions. J Vasc Interv Radiol. 2017;28:1–15.
Gaba RC, Lewandowski RJ, Hickey R, et al. Transcatheter therapy for hepatic malignancy: standardization of terminology and reporting criteria. J Vasc Interv Radiol. 2016;27:457–73.
Pernot S, Artru P, Mithieux F, et al. Complete pathological response of unresectable liver metastases from colorectal cancer after trans-arterial chemoembolization with drug-eluting beads loaded with irinotecan (DEBIRI) and concomitant systemic FOLFOX: a case report from the FFCD 1201 trial. Clin Res Hepatol Gastroenterol. 2015;39:e73–7.
Savic LJ, Chapiro J, Geschwind JH. Intra-arterial embolotherapy for intrahepatic cholangiocarcinoma: update and future prospects. Hepatobiliary Surg Nutr. 2017;6:7–21.
Tognolini A, Louie JD, Hwang GL, Hofmann LV, Sze DY, Kothary N. Utility of C-arm CT in patients with hepatocellular carcinoma undergoing transhepatic arterial chemoembolization. J Vasc Interv Radiol. 2010;21:339–47.
Wallace MJ, Murthy R, Kamat PP, et al. Impact of C-arm CT on hepatic arterial interventions for hepatic malignancies. J Vasc Interv Radiol. 2007;18:1500–7.
Kakeda S, Korogi Y, Ohnari N, et al. Usefulness of cone-beam volume CT with flat panel detectors in conjunction with catheter angiography for transcatheter arterial embolization. J Vasc Interv Radiol. 2007;18:1508–16.
Bapst B, Lagadec M, Breguet R, Vilgrain V, Ronot M. Cone beam computed tomography (CBCT) in the field of interventional oncology of the liver. Cardiovasc Intervent Radiol. 2016;39:8–20.
Zheng J, Li J, Cui X, Ye H, Ye L. Comparison of diagnostic sensitivity of C-arm CT, DSA and CT in detecting small HCC. Hepatogastroenterology. 2013;60:1509–12.
Wang Z, Chen R, Duran R, et al. Intraprocedural 3D quantification of lipiodol deposition on cone-beam CT predicts tumor response after transarterial chemoembolization in patients with hepatocellular carcinoma. Cardiovasc Intervent Radiol. 2015;38:1548–56.
Miyayama S, Yamashiro M, Hattori Y, et al. Efficacy of cone-beam computed tomography during transcatheter arterial chemoembolization for hepatocellular carcinoma. Jpn J Radiol. 2011;29:371–7.
Miyayama S, Yamashiro M, Hashimoto M, et al. Identification of small hepatocellular carcinoma and tumor-feeding branches with cone-beam CT guidance technology during transcatheter arterial chemoembolization. J Vasc Interv Radiol. 2013;24:501–8.
Pung L, Ahmad M, Mueller K, et al. The role of cone-beam CT in transcatheter arterial chemoembolization for hepatocellular carcinoma: a systematic review and meta-analysis. J Vasc Interv Radiol. 2017;28:334–41.
Mu L, Chapiro J, Stringam J, Geschwind JF. Interventional oncology in hepatocellular carcinoma: progress through innovation. Cancer J. 2016;22:365–72.
Schernthaner RE, Lin M, Duran R, Chapiro J, Wang Z, Geschwind J-F. Delayed-phase cone-beam CT improves detectability of intrahepatic cholangiocarcinoma during conventional transarterial chemoembolization. Cardiovasc Intervent Radiol. 2015;38:929–36.
Kahn J, Kaul D, Boning G, et al. Quality and dose optimized CT trauma protocol–recommendation from a university level-I trauma center. Rofo. 2017;189:844–54.
Grupp U, Schafer ML, Meyer H, et al. Reducing radiation dose in emergency CT scans while maintaining equal image quality: just a promise or reality for severely injured patients? Emerg Med Int. 2013;2013:984645.
Brook OR, Gourtsoyianni S, Brook A, Siewert B, Kent T, Raptopoulos V. Split-bolus spectral multidetector CT of the pancreas: assessment of radiation dose and tumor conspicuity. Radiology. 2013;269:139–48.
Scialpi M, Palumbo B, Pierotti L, et al. Detection and characterization of focal liver lesions by split-bolus multidetector-row CT: diagnostic accuracy and radiation dose in oncologic patients. Anticancer Res. 2014;34:4335–44.
Scialpi M, Pierotti L, Gravante S, et al. Split-bolus multidetector-row computed tomography technique for characterization of focal liver lesions in oncologic patients. Iran J Radiol. 2016;13:e20143.
Jonczyk M, Chapiro J, Collettini F, et al. Diagnostic accuracy of split-bolus single-phase contrast-enhanced cone-beam CT for the detection of liver tumors before transarterial chemoembolization. J Vasc Interv Radiol. 2017;28:1378–85.
Miyayama S, Yamashiro M, Okuda M, et al. Usefulness of cone-beam computed tomography during ultraselective transcatheter arterial chemoembolization for small hepatocellular carcinomas that cannot be demonstrated on angiography. Cardiovasc Intervent Radiol. 2009;32:255–64.
Loffroy R, Lin M, Rao P, et al. Comparing the detectability of hepatocellular carcinoma by C-arm dual-phase cone-beam computed tomography during hepatic arteriography with conventional contrast-enhanced magnetic resonance imaging. Cardiovasc Intervent Radiol. 2012;35:97–104.
Boning G, Kahn JF, Kaul D, et al. CT follow-up in patients with neuroendocrine tumors (NETs): combined radiation and contrast dose reduction. Acta Radiol. 2018;59:517–26. https://doi.org/10.1177/0284185117726101.
Schernthaner RE, Chapiro J, Sahu S, et al. Feasibility of a modified cone-beam CT rotation trajectory to improve liver periphery visualization during transarterial chemoembolization. Radiology. 2015;277:833–41.
Tacher V, Radaelli A, Lin M, Geschwind JF. How I do it: cone-beam CT during transarterial chemoembolization for liver cancer. Radiology. 2015;274:320–34.
Schernthaner RE, Duran R, Chapiro J, Wang Z, Geschwind J-FH, Lin M. A new angiographic imaging platform reduces radiation exposure for patients with liver cancer treated with transarterial chemoembolization. Eur Radiol. 2015;25:3255–62.
Louie JD, Kothary N, Kuo WT, et al. Incorporating cone-beam CT into the treatment planning for yttrium-90 radioembolization. J Vasc Interv Radiol. 2009;20:606–13.
Pellerin O, Lin M, Bhagat N, Shao W, Geschwind JF. Can C-arm cone-beam CT detect a micro-embolic effect after TheraSphere radioembolization of neuroendocrine and carcinoid liver metastasis? Cancer Biother Radiopharm. 2013;28:459–65.
Derbel H, Kobeiter H, Pizaine G, et al. Accuracy of a cone-beam CT virtual parenchymal perfusion algorithm for liver cancer targeting during intra-arterial therapy. J Vasc Interv Radiol. 2018;29(254–61):e2.
Acknowledgements
Dr. Martin Jonczyk and Dr. Federico Collettini participate in the BIH‐Charité Clinical Scientist Program (DM.BIH-04.15) funded by the Charité – Universitätsmedizin Berlin and the Berlin Institute of Health.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interests
MJ reports Grants from BIH Clinical Scientist and Philips Healthcare during the conduct of the study; DG reports personal fees from Bayer AG during the conduct of the study; BH reports Grants from Philips Healthcare, Bayer AG, GE, Siemens and Terumo during the conduct of the study. All other authors have nothing to disclose in relation to this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Jonczyk, M., Collettini, F., Schnapauff, D. et al. Visibility of Hypovascularized Liver Tumors during Intra-Arterial Therapy Using Split-Bolus Single-Phase Cone Beam CT. Cardiovasc Intervent Radiol 42, 260–267 (2019). https://doi.org/10.1007/s00270-018-2101-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-018-2101-2