
Abstract
Introduction
Patients undergoing unilateral adrenalectomy for primary aldosteronism (PA) may have a solitary adenoma, unilateral hyperplasia, or multiple adenomas on final pathology. This study investigated whether the underlying pathological diagnosis was associated with differences in clinical presentation and postoperative outcomes.
Methods
A retrospective cohort study of patients undergoing unilateral adrenalectomy for PA from 2004 to 2015 at our institution was performed. Baseline clinical and laboratory parameters, as well as postoperative biochemical and hypertension cure rates, were compared across the three aforementioned pathological groups.
Results
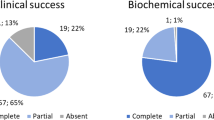
Of 206 patients who met criteria for inclusion, 152 (73.8%) had a single adenoma, 33 (16%) had unilateral hyperplasia, and 21 (10.2%) had multiple unilateral adenomas. Patients with unilateral hyperplasia were more likely to be male (81.2% vs 57.9%, P = .03), undergo left-sided adrenalectomy (78.8% vs 47.4%, P < .01), and had a lower median adrenal venous sampling lateralization index (9.8 vs 19.8, P = .04) compared to those with solitary, but not multiple unilateral adenomas. No differences were seen in age, duration of hypertension, preoperative plasma aldosterone levels, plasma renin activities, 24-h urinary aldosterone excretion, serum potassium concentrations, and the number of preoperative antihypertensive medications across all three pathological groups. All patients achieved biochemical cure following adrenalectomy, and no significant differences in the rates of hypertension cure or improvement were observed in comparisons across pathological subtype.
Conclusions
Clinical presentation and postoperative outcomes are similar regardless of underlying pathology in patients with PA. Because one in four patients may harbor unilateral hyperplasia or multiple adenomas, total unilateral adrenalectomy should be performed as the operation of choice over adrenal-sparing approaches.

Similar content being viewed by others


References
Young WF (2007) Primary aldosteronism: renaissance of a syndrome. Clin Endocrinol (Oxf) 66(5):607–618
Funder JW, Carey RM, Mantero F et al (2016) The management of primary aldosteronism: case detection, diagnosis, and treatment: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 101(5):1889–1916
Milliez P, Girerd X, Plouin PF et al (2005) Evidence for an increased rate of cardiovascular events in patients with primary aldosteronism. J Am Coll Cardiol 45(8):1243–1248
Rossi GP, Bernini G, Desideri G et al (2006) Renal damage in primary aldosteronism: results of the PAPY study. Hypertension 48(2):232–238
Rossi GP, Sechi LA, Giacchetti G et al (2008) Primary aldosteronism: cardiovascular, renal and metabolic implications. Trends Endocrinol Metab 19(3):88–90
Quillo AR, Grant CS, Thompson GB et al (2011) Primary aldosteronism: results of adrenalectomy for nonsingle adenoma. J Am Coll Surg 213(1):106–112
Trésallet C, Salepçioglu H, Godiris-Petit G et al (2010) Clinical outcome after laparoscopic adrenalectomy for primary hyperaldosteronism: the role of pathology. Surgery 148(1):129–134
Novitsky YW, Kercher KW, Rosen MJ et al (2005) Clinical outcomes of laparoscopic adrenalectomy for lateralizing nodular hyperplasia. Surgery 138(6):1009–1017
Morioka M, Kobayashi T, Sone A et al (2008) Primary aldosteronism due to unilateral adrenal hyperplasia. Report of two cases and review of the literature. Endocr J 47(4):443–449
Iacobone M, Citton M, Viel G et al (2012) Unilateral adrenal hyperplasia: a novel cause of surgically correctable primary hyperaldosteronism. Surgery 152(6):1248–1255
Leung A, Sasano H, Nishikwa T et al (2013) Multiple unilateral adrenal adenomas in a patient with primary hyperaldosteronism. Endocr Pract 14(1):76–79
Hashimoto N, Kawamura Y, Nakamura T et al (2011) A case of primary aldosteronism caused by multiple adrenocortical macronodules. Intern Med 50(6):585–590
Stowasser M, Gordon RD (2013) The renaissance of primary aldosteronism: What has it taught us? Hear Lung Circ 22(6):412–420
Walz MK, Gwosdz R, Levin SL et al (2008) Retroperitoneoscopic adrenalectomy in Conn’s syndrome caused by adrenal adenomas or nodular hyperplasia. World J Surg 32(5):847–853. https://doi.org/10.1007/s00268-008-9513-0
Sigurjonsdottir HA, Gronowitz M, Andersson O et al (2012) Unilateral adrenal hyperplasia is a usual cause of primary hyperaldosteronism. Results from a Swedish screening study. BMC Endocr Disord 12:17
Weisbrod AB, Webb RC, Mathur A et al (2013) Adrenal histologic findings show no difference in clinical presentation and outcome in primary hyperaldosteronism. Ann Surg Oncol 20(3):753–758
Obara T, Ito Y, Okamoto T et al (1992) Risk factors associated with postoperative persistent hypertension in patients with primary aldosteronism. Surgery 112(6):987–993
Ito Y, Fujimoto Y, Obara T, Kodama T (1990) Clinical significance of associated nodular lesions of the adrenal in patients with aldosteronoma. World J Surg 14(3):330–334. https://doi.org/10.1007/BF01658518
Hennings J, Andreasson S, Botling J et al (2010) Long-term effects of surgical correction of adrenal hyperplasia and adenoma causing primary aldosteronism. Langenbeck’s Arch Surg 395(2):133–137
Gioco F, Seccia TM, Gomez-Sanchez EP et al (2015) Adrenal histopathology in primary aldosteronism: Is it time for a change? Hypertension 66(4):724–730
Mete O, Duan K (2018) The many faces of primary aldosteronism and cushing syndrome: a reflection of adrenocortical tumor heterogeneity. Front Med 5:54
Young WF, Stanson AW (2009) What are the keys to successful adrenal venous sampling (AVS) in patients with primary aldosteronism? Clin Endocrinol (Oxf) 70(1):14–17
Zhang Z, Meng H, Hou Z et al (2013) Fetal adrenal gland in the second half of gestation: morphometrical assessment with 3.0T post-mortem MRI. PLoS ONE 8(10):e75511
Lam KY, Chan ACL, Lo CY (2001) Morphological analysis of adrenal glands: a prospective analysis. Endocr Pathol 12(1):33–38
Katayama Y, Takata N, Tamura T et al (2005) A case of primary aldosteronism due to unilateral adrenal hyperplasia. Hypertens Res 28(4):379–384
Proye CAG, Mulliez EAR, Carnaille BML et al (1998) Essential hypertension: first reason for persistent hypertension after unilateral adrenalectomy for primary aldosteronism? Surgery 124(6):1128–1133
Walz MK, Peitgen K, Saller B et al (1998) Subtotal adrenalectomy by the posterior retroperitoneoscopic approach. World J Surg 22(6):621–627. https://doi.org/10.1007/s002689900444
Ishidoya S, Ito A, Sakai K et al (2005) Laparoscopic partial versus total adrenalectomy for aldosterone producing adenoma. J Urol 174(1):40–43
Nanba AT, Nanba K, Byrd JB et al (2017) Discordance between imaging and immunohistochemistry in unilateral primary aldosteronism. Clin Endocrinol (Oxf) 87(6):665–672
Volpe C, Hamberger B, Höög A et al (2015) Primary aldosteronism: functional histopathology and long-term follow-up after unilateral adrenalectomy. Clin Endocrinol (Oxf) 82(5):639–647
Swearingen AJ, Kahramangil B, Monteiro R et al (2018) Analysis of postoperative biochemical values and clinical outcomes after adrenalectomy for primary aldosteronism. Surgery 163(4):807–810
Kline GA, Darras P, Leung AA et al (2018) Surprisingly low aldosterone levels in peripheral veins following intravenous sedation during adrenal vein sampling. J Hypertens 37(3):596–602
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Shariq, O.A., Mehta, K., Thompson, G.B. et al. Primary Aldosteronism: Does Underlying Pathology Impact Clinical Presentation and Outcomes Following Unilateral Adrenalectomy?. World J Surg 43, 2469–2476 (2019). https://doi.org/10.1007/s00268-019-05059-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-019-05059-y