
Abstract
Objective
Therapeutic lateral neck dissection (ND) is recommended for N1b papillary thyroid carcinoma (PTC), while prophylactic contralateral lateral ND is not. Given the paucity of data, we investigated the frequency of and risk factors for occult lymph node metastases (LNM) in the contralateral lateral neck for N1b patients.
Patients and methods
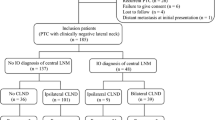
This is a retrospective study conducted at a cancer center. Inclusion criteria were: unilateral PTC and ipsilateral lateral LNM confirmed by fine-needle aspiration biopsy. Patients with contralateral lateral LNM or bilateral tumor on ultrasound were excluded. All patients were treated with total thyroidectomy, bilateral central ND, ipsilateral therapeutic lateral ND and prophylactic contralateral ND of levels III–IV, followed by radioactive iodine.
Results
Sixty-three patients met the inclusion criteria. Occult contralateral lateral LNM were found in 23/63 patients (36.5%) who had more LNM in ispilateral (p = .01) and contralateral level VI (p < .0001), more frequent microscopic tumor in the contralateral lobe (p = .017) and a trend toward being at high risk (p = .06). Using receiver operating characteristic analysis, a cutoff of >4 LNM in ipsilateral level VI optimized sensitivity and specificity for predicting contralateral lateral LNM, with a sensitivity of 74%, specificity of 65%, positive predictive value of 55% and negative predictive value of 81%. Neck recurrence occurred in 14%, with only 1 patient recurring only in the contralateral lateral neck (1.5%).
Conclusion
Occult LNM in the contralateral lateral neck was found in 36.5% of patients. Five or more ipsilateral central LNM may aid in predicting contralateral lateral LNM, and high-risk patients may be more at risk. The clinical benefit of prophylactic contralateral lateral ND remains doubtful, however.

Similar content being viewed by others


References
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE et al (2015) American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 26(1):1–133
Carty SE, Cooper DS, Doherty GM, Duh Q-Y, Kloos RT, Mandel SJ et al (2009) Consensus statement on the terminology and classification of central neck dissection for thyroid cancer. Thyroid 19(11):1153–1158
Robbins KT, Shaha AR, Medina JE, Califano JA, Wolf GT, Ferlito A et al (2008) Consensus statement on the classification and terminology of neck dissection. Arch Otolaryngol Head Neck Surg 134(5):536–538
Tuttle RM, Tala H, Shah J, Leboeuf R, Ghossein R, Gonen M et al (2010) Estimating risk of recurrence in differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnant ablation: using response to therapy variables to modify the initial risk estimates predicted by the new American thyroid association staging system. Thyroid 20(12):1341–1349
Ito Y, Miyauchi A (2009) Prognostic factors and therapeutic strategies for differentiated carcinomas of the thyroid. Endocr J 56(2):177–192
Ito Y, Kudo T, Kobayashi K, Miya A, Ichihara K, Miyauchi A (2012) Prognostic factors for recurrence of papillary thyroid carcinoma in the lymph nodes, lung, and bone: analysis of 5,768 patients with average 10-year follow-up. World J Surg 36(6):1274–1278. https://doi.org/10.1007/s00268-012-1423-5
Jeon MJ, Kim WG, Jang EK, Choi YM, Song DE, Sung TY et al (2015) Sub-classification of lateral cervical lymph node metastasis in papillary thyroid carcinoma by pathologic criteria. PLoS ONE 10(7):1–12
Sugitani I, Fujimoto Y, Yamada K, Yamamoto N (2008) Prospective outcomes of selective lymph node dissection for papillary thyroid carcinoma based on preoperative ultrasonography. World J Surg 32(11):2494–2502. https://doi.org/10.1007/s00268-008-9711-9
Wang LY, Palmer FL, Nixon IJ, Tuttle RM, Shah JP, Patel SG et al (2015) Lateral neck lymph node characteristics prognostic of outcome in patients with clinically evident N1b papillary thyroid cancer. Ann Surg Oncol 22(11):3530–3536
Hughes DT, Miller BS, Cohen MS, Doherty GM, Gauger PG (2014) Outcomes of total thyroidectomy with therapeutic central and lateral neck dissection with a single dose of radioiodine in the treatment of regionally advanced papillary thyroid cancer and effects on serum thyroglobulin. Ann Surg Oncol 21(5):1647–1652
Lango M, Flieder D, Arrangoiz R, Veloski C, Yu JQ, Li T et al (2013) Extranodal extension of metastatic papillary thyroid carcinoma: correlation with biochemical endpoints, nodal persistence, and systemic disease progression. Thyroid 23(9):1099–1105
McNamara WF, Wang LY, Palmer FL, Nixon IJ, Shah JP, Patel SG et al (2016) Pattern of neck recurrence after lateral neck dissection for cervical metastases in papillary thyroid cancer. Surgery 159(6):1565–1571
Chéreau N, Buffet C, Trésallet C, Tissier F, Leenhardt L, Menegaux F (2016) Recurrence of papillary thyroid carcinoma with lateral cervical node metastases: predictive factors and operative management. Surgery 159(3):755–762
Ito Y, Kudo T, Takamura Y, Kobayashi K, Miya A, Miyauchi A (2012) Lymph node recurrence in patients with N1b papillary thyroid carcinoma who underwent unilateral therapeutic modified radical neck dissection. World J Surg 36(3):593–597. https://doi.org/10.1007/s00268-011-1391-1
Keum HS, Ji YB, Kim JM, Jeong JH, Choi WH, Ahn YH et al (2012) Optimal surgical extent of lateral and central neck dissection for papillary thyroid carcinoma located in one lobe with clinical lateral lymph node metastasis. World J Surg Oncol 10:221
Société Française d’Oto-rhino-laryngologie et de Chirurgie de la Face et du Cou. Prise en charge ganglionnaire dans les cancers differenciés de souche folliculaire du corps thyroïdien chez l’adulte (2012)
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest.
Rights and permissions
About this article

Cite this article
Bohec, H., Breuskin, I., Hadoux, J. et al. Occult Contralateral Lateral Lymph Node Metastases in Unilateral N1b Papillary Thyroid Carcinoma. World J Surg 43, 818–823 (2019). https://doi.org/10.1007/s00268-018-4862-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-018-4862-9