
Abstract
Objective
To estimate the improvement in surgical exposure by removal of the coccyx, during abdomino-perineal resection (APR), in rectal cancer patients.
Methods
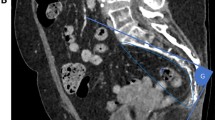
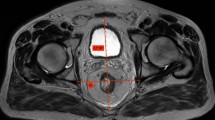
Retrospective study of 29 consecutive patients with rectal cancer was carried out. Using MR T2 sagittal series, the solid angle was estimated using the angle determined by the anterior resection margin and the tip of coccyx (no coccyx resection) or the tip of last sacral vertebra (coccyx resection). The solid angle provides an estimate of the tridimensional surface area provided by an original angle resulting in the best estimate of the surgeon’s view/exposure to the critical dissecting point of choice (anterior rectal wall). The difference (“Gain”) in surgical field exposure by removal of the coccyx was compared by the solid angle variation between the two estimates (with and without the coccyx).
Results
Routine removal of the coccyx determines an average 42% (95% CI 27–57%) gain in surgical field exposure area facing the anterior rectal wall at the level of the prostate/vagina by the surgeon. Fifteen (51%) patients had ≥30% (median) estimated gain in surgical field exposure by coccygectomy. There was no association between BMI, age or gender and estimated gain in surgical field exposure area.
Conclusions
Routine removal of the coccyx during APR may result in an average increase in 42% in surgical field exposure during APR’s perineal dissection. Precise estimation of surgical field exposure gain by removal of the coccyx may be predicted by MR sagittal series for each individual patient.



Similar content being viewed by others

References
Nagtegaal ID, van de Velde CJ, Marijnen CA et al (2005) Low rectal cancer: a call for a change of approach in abdominoperineal resection. J Clin Oncol 23:9257–9264
Bosch SL, Nagtegaal ID (2012) The importance of the pathologist’s role in assessment of the quality of the mesorectum. Curr Colorectal Cancer Rep 8:90–98
Shihab OC, Brown G, Daniels IR et al (2010) Patients with low rectal cancer treated by abdominoperineal excision have worse tumors and higher involved margin rates compared with patients treated by anterior resection. Dis Colon Rectum 53:53–56
How P, Shihab O, Tekkis P et al (2011) A systematic review of cancer related patient outcomes after anterior resection and abdominoperineal excision for rectal cancer in the total mesorectal excision era. Surg Oncol 20:e149–155
Prytz M, Angenete E, Bock D et al (2016) Extralevator abdominoperineal excision for low rectal cancer-extensive surgery to be used with discretion based on 3-year local recurrence results: a registry-based, observational national cohort study. Ann Surg 263:516–521
de Campos-Lobato LF, Stocchi L, Dietz DW et al (2011) Prone or lithotomy positioning during an abdominoperineal resection for rectal cancer results in comparable oncologic outcomes. Dis Colon Rectum 54:939–946
Sao Juliao GP, Ortega CD, Vailati BB et al (2017) Magnetic resonance imaging following neoadjuvant chemoradiation and transanal endoscopic microsurgery for rectal cancer—key diagnostic features of local recurrences. Colorectal Dis 19:O196–O203
Brown G, Daniels IR, Richardson C et al (2005) Techniques and trouble-shooting in high spatial resolution thin slice MRI for rectal cancer. Br J Radiol 78:245–251
Habr-Gama A, Sao Juliao GP, Mattacheo A et al (2017) Extralevator abdominal perineal excision versus standard abdominal perineal excision: impact on quality of the resected specimen and postoperative morbidity. World J Surg. https://doi.org/10.1007/s00268-017-3963-1
Naito M (1957) A method of calculating the solid angle subtended by a circular aperture. J Phys Soc Jpn 12:1122–1129
Shihab OC, How P, West N et al (2011) Can a novel MRI staging system for low rectal cancer aid surgical planning? Dis Colon Rectum 54:1260–1264
West NP, Anderin C, Smith KJ et al (2010) Multicentre experience with extralevator abdominoperineal excision for low rectal cancer. Br J Surg 97:588–599
Shihab OC, Heald RJ, Holm T et al (2012) A pictorial description of extralevator abdominoperineal excision for low rectal cancer. Colorectal Dis 14:e655–660
Taylor FG, Quirke P, Heald RJ et al (2011) Preoperative high-resolution magnetic resonance imaging can identify good prognosis stage I, II, and III rectal cancer best managed by surgery alone: a prospective, multicenter, European study. Ann Surg 253:711–719
Wang YL, Dai Y, Jiang JB et al (2015) Application of laparoscopic extralevator abdominoperineal excision in locally advanced low rectal cancer. Chin Med J (Engl) 128:1340–1345
Han JG, Wang ZJ, Qian Q et al (2014) A prospective multicenter clinical study of extralevator abdominoperineal resection for locally advanced low rectal cancer. Dis Colon Rectum 57:1333–1340
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
São Julião, G.P., Ortega, C.D., Vailati, B.B. et al. The Estimate of the Impact of Coccyx Resection in Surgical Field Exposure During Abdominal Perineal Resection Using Preoperative High-Resolution Magnetic Resonance. World J Surg 42, 3765–3770 (2018). https://doi.org/10.1007/s00268-018-4683-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-018-4683-x