
Abstract
Background
Propofol is has been widely used for sedation in the field of esthetic surgery because of its favorable pharmacokinetic profile. Propofol sedation-induced side effects are rare. However, when present, they can be serious. The number of malpractice claims associated with propofol sedation has increased in recent years. This study aims to show which procedures lead to the most claims in the field of esthetic surgery through a review of Korean precedents.
Methods
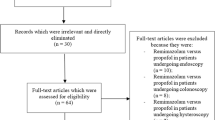
Thirteen precedent cases of propofol sedation in the field of esthetic surgery were collected between 2000 and 2016. We analyzed the type of procedure, administration route, anesthesia provider, complications, timing of damaging events, average indemnification, plaintiff’s (patients) winning rate, ratio and the reason of limitation of liability and the key factors affecting the judgement in these cases.
Results
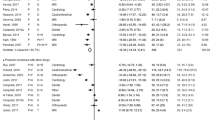
Most plaintiffs were women, and in most cases (11/13, 73.3%), the times of the damaging events were in maintenance and the anesthesia provider was the surgeon. The most common complication related to propofol sedation was hypoxic brain damage. Among the 13 cases, 12 were won by the plaintiff. The mean claim settlement was 339,455,814 KRW (USD 301,792.15). The key factors affecting the judgement were administration method and staff, monitoring method, preparation of emergency kit, response to emergencies, transfer to a higher-level hospital, detailed medical recording about event and informed consent.
Conclusion
The number of claims owing to propofol sedation after esthetic surgery is increasing. Close monitoring during the operation, immediate reaction to an event and thorough medical records were main key factors that influenced the judgement. Preoperative explanation about the possibility of complications was important. The findings will help surgeons achieve high patient satisfaction and reduce liability concerns.
Level of Evidence V
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.






Similar content being viewed by others

References
Rex DK (2006) Review article: moderate sedation for endoscopy: sedation regimens for non-anaesthesiologists. Aliment Pharmacol Ther 24:163–171
Aisenberg J, Cohen LB, Piorkowski JD Jr (2007) Propofol use under the direction of trained gastroenterologists: an analysis of the medicolegal implications. Am J Gastroenterol 102(4):707–713
Lee SA, Lee MS, Kim YA, Ahn WS, Lee HC (2010) Propofol abuse of the medical personnel in operation room in Korea. Korean J Leg Med 34:101–107
Eger EI (2004) Characteristics of anesthetic agents used for induction and maintenance of general anesthesia. Am J Health Syst Pharm Res 61:3–10
Brown TB, Lovato LM, Parker D (2005) Procedural sedation in the acute care setting. Am Fam Physician 71(1):85–90
Roh WS, Kim DK, Jeon YH, Kim SH, Lee SC, Ko YK, Lee YC, Lee GH (2015) Analysis of anesthesia-related medical disputes in the 2009–2014 period using the Korean Society of Anesthesiologists database. J Korean Med Sci 30(2):207–213
White AA, Pichert JW, Bledsoe SH, Irwin C, Entman SS (2005) Cause and effect analysis of closed claims in obstetrics and gynecology. Obstet Gynecol 105:1031–1038
Ward CJ (1991) Analysis of 500 obstetric and gynecologic malpractice claims: causes and prevention. Am J Obstet Gynecol 165:298e306
Wani S, Azar R, Hovis CE, Hovis RM, Cote GA, Hall M, Waldbaum L, Kushnir V, Early D, Mullady DK, Murad F, Edmundowicz SA, Jonnalagadda SS (2008) Obesity as a risk factor for sedation-related complications during propofol-mediated sedation for advanced endoscopic procedures. Scand J Gastroenterol 43(3):368–374
Statement on safe use of propofol (2014). www.asahq.org/…/statement-on-safe-use-of-propofol.pdf Accessed 13 Oct 2017
Kang H, Kim DK, Choi YS, Yoo YC, Chung HS (2016) Practice guidelines for propofol sedation by non-anesthesiologists: the Korean Society of anesthesiologists task force recommendations on propofol sedation. Korean J Anesthesiol 69(6):545–554
Cohen LB, Dubovsky AN, Aisenberg J et al (2003) Propofol for endoscopic sedation: a protocol for safe and effective administration by the gastroenterologist. Gastrointest Endosc 58:725–732
Chutkan R, Cohen J, Abedi M, Correa MC, Dominitz J, Gersin K, Greenwald D, Kantsevoy S, Kowdley K, Nguyen M, Roy Soetikno R, Telford J, Vargo J (2004) Training guideline for use of propofol in gastrointestinal endoscopy. Gastrointest Endosc 60:167–172
Lee JK, Jang DK, Kin WH, Kim JW, Jang BI (2017) Safety of non-anesthesiologist administration of propofol for gastrointestinal endoscopy. Korean J Gastroenterol 69(1):55–58. https://doi.org/10.4166/kjg.2017.69.1.55
Shin SH, Kim SY, Jang SG, Lee W (2017) Analysis of closed medical litigation in urology. Investig Clin Urol. 58(5):317–323
Acknowledgements
None of the authors has a financial interest in any of the products, devices or drugs mentioned in this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no potential conflicts of interest to disclose.
Rights and permissions
About this article

Cite this article
Lee, D.H., Woo, J.H. & Hong, S.E. Judicial Precedent-Based Clinical Practice Guidelines of Propofol in Sedative Esthetic Surgery. Aesth Plast Surg 42, 891–898 (2018). https://doi.org/10.1007/s00266-018-1122-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-018-1122-1