
Abstract
Purpose
We investigated the various impingement angles (including both bony and prosthetic impingement) and impingement types that can occur after THA, even when the same combined anteversion parameter is used. We also investigated the relationship between impingement angle and acetabular morphology or femoral anteversion.
Methods
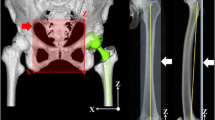
We evaluated 83 patients with no hip arthritis. We divided them into six groups according to acetabular CE angle (≤15°, >15–≤25°, and >25°) and femoral anteversion (≤20° and >20°). Using three-dimensional templating software, we changed stem and cup anteversion to satisfy a combined anteversion (CA) of 50° in each hip (stem anteversion + cup anteversion = 50°) and investigated the resulting impingement angles.
Results
Even with the same CA, differences in impingement angle occurred: 18.3° ± 7.2° with flexion, 30.2° ± 9.7° with internal rotation at 90° flexion, 20.2° ± 12.5° with extension, and 26.2° ± 7.8° with external rotation. As stem anteversion increased, the impingement type changed from prosthetic impingement to bony impingement in flexion and internal rotation and from bony impingement to prosthetic impingement in extension and external rotation. The flexion angle and internal rotation angle at 90° flexion increased (p < 0.016) as CE angle decreased. There were no significant differences between high and low femoral anteversion.
Conclusions
Combined anteversion theory should be used with care because of large differences in impingement angles. A stem anteversion of 30° and cup anteversion of 20° appear to be ideal for obtaining a larger impingement angle under this condition.





Similar content being viewed by others

References
Grinten M, Verhaar JAN (2003) Dislocation of total hip prostheses: risk factors and treatment. Ned Tijdschr Gen 147:286–290
Coventry MB (1985) Late dislocations in patients with Charnley total hip arthroplasty. J Bone Joint Surg Am 67:832–841
Harris WH (1980) Advances in surgical technique for total hip replacement: without and with osteotomy of the greater trochanter. Clin Orthop Relat Res 146:188–204
Lewinnek GE, Lewis JL, Tarr R et al (1978) Dislocations after total hip replacement arthroplasties. J Bone Joint Surg Am 60:217–220
Widmer KH, Zurfluh B (2004) Compliant positioning of total hip components for optimal range of motion. J Orthop Res 22:815–821
Masaoka T, Yamamoto K, Shishido T et al (2006) Study of hip joint dislocation after total hip arthroplasty. Int Orthop 30:26–30
Nakashima Y, Hirata M, Akiyama M et al (2014) Combined anteversion technique reduced the dislocation in cementless total hip arthroplasty. Int Orthop 38:27–32
Kessler O, Patil S, Wirth S et al (2008) Bony impingement affects range of motion after total hip arthroplasty: A subject-specific approach. J Orthop Res 26:443–452
Suzuki K, Matsubara M, Morita S et al (2002) CT image evaluation of the internal rotation limit prior to bony impingement after total hip arthroplasty. J Orthop Sci 7:433–438
Bartz RL, Nobel PC, Kadakia NR et al (2000) The effect of femoral component head size on posterior dislocation of the artificial hip joint. J Bone Joint Surg Am 82:1300–1307
Inoue K, Wicart P, Kawasaki T et al (2000) Prevalence of hip osteoarthritis and acetabular dysplasia in french and japanese adults. Rheumatology 39:745–748
Sugano N, Noble PC, Kamaric E et al (1998) The morphology of the femur in developmental dysplasia of the hip. J Bone Joint Surg Br 80:711–719
Australian Registry (2016) Australian Orthopaedic Association National Joint Replacement Registry annual report 2016. https://aoanjrr.sahmri.com/annual-reports-2016. Accessed 02 October 2017
The New Zealand Joint Registry (2016) New Zealand Orthopaedic Association 17 year report. https://nzoa.org.nz/nz-joint-registry. Accessed 02 October 2017
Ranawat CS, Maynard MJ (1991) Modern techniques of cemented total hip arthroplasty. Tech Orthop 6:17–25
Dorr LD, Malik A, Dastane M et al (2009) Combined anteversion technique for total hip arthroplasty. Clin Orthop Relat Res 467:119–127
Jolles BM, Zangger P, Leyvraz PF (2002) Factors predisposing to dislocation after primary total hip arthroplasty: a multivariate analysis. J Arthroplast 17:282–288
Fujishiro T, Hiranaka T, Hashimoto S et al (2016) The effect of acetabular and femoral component version on dislocation in primary total hip arthroplasty. Int Orthop 40:697–702
Shoji T, Yasunaga Y, Yamasaki T et al (2013) Bony impingement depends on the bone morphology of the hip after total hip arthroplasty. Int Orthop 37:1897–1903
Iftach H, Lazaros P, Asheesh B et al (2013) Anterior inferior iliac spine morphology correlates with hip range of motion: a classification system and dynamic model. Clin Orthop Relat Res 471:2497–2503
Shoji T, Yasunaga Y, Yamasaki T et al (2015) Low femoral antetorsion as a risk factor for bony impingement after bipolar hemiarthroplasty. J Orthop Surg Res. https://doi.org/10.1186/s13018-015-0248-y. Accessed 02 October 2017
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ohmori, T., Kabata, T., Kajino, Y. et al. Differences in range of motion with the same combined anteversion after total hip arthroplasty. International Orthopaedics (SICOT) 42, 1021–1028 (2018). https://doi.org/10.1007/s00264-017-3653-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-017-3653-5