
Abstract
Background
Pectus excavatum results from dorsal deviation of the sternum causing narrowing of the anterior-posterior diameter of the chest. It can result in significant cosmetic deformities and cardiopulmonary compromise if severe. The Nuss procedure is a minimally invasive technique that involves placing a thin horizontally oriented metal bar below the dorsal sternal apex for correction of the pectus deformity.
Objective
To identify the frequency and types of Nuss bar migrations, to present a new categorization of bar migrations, and to present examples of true migrations and pseudomigrations.
Materials and methods
We retrospectively reviewed the electronic medical records and all pertinent radiologic studies of 311 pediatric patients who underwent a Nuss procedure. We evaluated the frequency and type of bar migrations.
Results
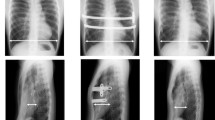
Bar migration was demonstrated in 23 of 311 patients (7%) and occurred within a mean period of 26 days after surgery. Bar migrations were subjectively defined as deviation of the bar from the position demonstrated on the immediate postoperative radiographs and categorized as superior, inferior, rotation, lateral or flipped using a new classification system. Sixteen of the 23 migrations required re-operation.
Conclusion
Nuss bar migration can be diagnosed with careful evaluation of serial radiographs. Nuss bar migration has a wide variety of appearances and requires exclusion of pseudomigration resulting from changes in patient positioning between radiologic examinations.











Similar content being viewed by others


References
Hebra A (2009) Minimally invasive repair of pectus excavatum. Semin Thorac Cardiovasc Surg 21:76–84
Kotzot D, Schwabegger AH (2009) Etiology of chest wall deformities — a genetic review for the treating physician. J Pediatr Surg 44:2004–2011
Ravitch MM (1977) Repair of pectus excavatum in children under 3 years of age: a twelve-year experience. Ann Thorac Surg 23:301
Quigley PM, Haller JA Jr, Jelus KL et al (1996) Cardiorespiratory function before and after corrective surgery in pectus excavatum. J Pediatr 128:638–643
Peterson RJ, Young WG Jr, Godwin JD et al (1985) Noninvasive assessment of exercise cardiac function before and after pectus excavatum repair. J Thorac Cardiovasc Surg 90:251–260
Fabricius J, Davidsen HG, Hansen AT (1957) Cardiac function in funnel chest; twenty-six patients investigated by cardiac catheterization. Dan Med Bull 4:251–257
Colombani PM (2009) Preoperative assessment of chest wall deformities. Semin Thorac Cardiovasc Surg 21:58–63
Ohno K, Morotomi Y, Nakahira M et al (2003) Indications for surgical repair of funnel chest based on indices of chest wall deformity and psychological state. Surg Today 33:662–665
Fokin AA, Steuerwald NM, Ahrens WA et al (2009) Anatomical, histologic, and genetic characteristics of congenital chest wall deformities. Semin Thorac Cardiovasc Surg 21:44–57
Robicsek F, Watts LT, Fokin AA (2009) Surgical repair of pectus excavatum and carinatum. Semin Thorac Cardiovasc Surg 21:64–75
Nuss D (2008) Minimally invasive surgical repair of pectus excavatum. Semin Pediatr Surg 17:209–217
Haller JA Jr, Kramer SS, Lietman SA (1987) Use of CT scans in selection of patients for pectus excavatum surgery: a preliminary report. J Pediatr Surg 22:904–906
Ravitch MM (1949) The operative treatment of pectus excavatum. Ann Surg 129:429–444
Gibreel W, Zendejas B, Joyce D et al (2016) Minimally invasive repairs of pectus excavatum: surgical outcomes, quality of life, and predictors of reoperation. J Am Coll Surg 222:245–252
Park HJ, Chung WJ, Lee IS et al (2008) Mechanism of bar displacement and corresponding bar fixation techniques in minimally invasive repair of pectus excavatum. J Pediatr Surg 43:74–78
Park HJ (2007) Technical innovations in the minimally invasive approach for treating pectus excavatum: a paradigm shift through six years’ experience with 630 patients. Innovations 2:25–28
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Rights and permissions
About this article

Cite this article
Binkovitz, L.E., Zendejas, B., Moir, C.R. et al. Nuss bar migrations: occurrence and classification. Pediatr Radiol 46, 1797–1803 (2016). https://doi.org/10.1007/s00247-016-3688-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-016-3688-6