
Abstract
Background
Breath-held two-dimensional balanced steady--state free precession cine acquisition (2-D breath-held SSFP), accelerated with parallel imaging, is the method of choice for evaluating ventricular function due to its superior blood-to-myocardial contrast, edge definition and high intrinsic signal-to-noise ratio throughout the cardiac cycle.
Objective
The purpose of this study is to qualitatively and quantitatively compare the two different single-breath-hold 3-D cine SSFP acquisitions using 1) multidirectional sensitivity encoding (SENSE) acceleration factors (3-D multiple SENSE SSFP), and 2) k-t broad-use linear acceleration speed-up technique (3-D k-t SSFP) with the conventional 2-D breath-held SSFP in non-sedated asymptomatic volunteers and children with single ventricle congenital heart disease.
Materials and methods
Our prospective study was performed on 30 non-sedated subjects (9 healthy volunteers and 21 functional single ventricle patients), ages 12.5 +/- 2.8 years. Two-dimensional breath-held SSFP with SENSE acceleration factor of 2, eight-fold accelerated 3-D k-t SSFP, and 3-D multiple SENSE SSFP with total parallel imaging factor of 4 were performed to evaluate ventricular volumes and mass in the short-axis orientation. Image quality scores (blood myocardial contrast, edge definition and interslice alignment) and volumetric analysis (end systolic volume, end diastolic volume and ejection fraction) were performed on the data sets by experienced users. Paired t-test was performed to compare each of the 3-D k-t SSFP and 3-D multiple SENSE SSFP clinical scores against 2-D breath-held SSFP. Bland-Altman analysis was performed on left ventricle (LV) and single ventricle volumetry. Interobserver and intraobserver variability in volumetric measurements were determined using intraclass coefficients.
Results
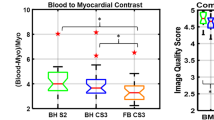
The clinical scores were highest for the 2-D breath-held SSFP images. Between the two 3-D sequences, 3-D multiple SENSE SSFP performed better than 3-D k-t SSFP. Bland-Altman analysis for volumes indicated that variability was more between 3-D k-t SSFP and 2-D breath-held SSFP acquisitions than between 3-D multiple SENSE SSFP and 2-D breath-held SSFP acquisitions. In the non-sedated population, interslice alignment scores were better for 3-D k-t SSFP and 3-D multiple SENSE SSFP than 2-D breath-held SSFP. The blood-myocardial contrast and edge definition scores were better for 2-D breath-held SSFP than 3-D k-t SSFP and 3-D multiple SENSE SSFP. Scan duration was shorter for 3-D acquisition sequences compared to the 2-D breath-held stack.
Conclusion
Three-dimensional k-t SSFP and 3-D multiple SENSE for ventricular volumetry release the constraints of multiple breath-holds in children and overcome problems related to interslice misalignment caused by inconsistent amplitude of breathing. Three-dimensional multiple SENSE SSFP performed better in our pediatric population than 3-D k-t SSFP. However, these 3-D sequences produce lower-quality diagnostic images than the gold standard 2-D breath-held SSFP sequence.





Similar content being viewed by others


Abbreviations
- 2-D breath-held SSFP:
-
2-dimensional breath-held steady-state free precession
- 3-D k-t SSFP:
-
3-dimensional k-t BLAST steady-state free precession
- 3-D multiple SENSE SSFP:
-
3-dimensional multiple SENSE steady-state free precession
- BLAST:
-
Broad-use Linear Acquisition Speed-up Technique
- EDV:
-
End-diastolic volume
- ESV:
-
End-systolic volume
- ICC:
-
Intraclass coefficient
- k-t:
-
K-space domain and time domain
- LV:
-
Left ventricle
- RF:
-
Radio frequency
- RV:
-
Right ventricle
- SENSE:
-
Sensitivity encoding
- SNR:
-
Signal-to-noise ratio
- SSFP:
-
Steady-state free precession
- VCG:
-
Vector electrocardiographic gating
References
Delgado JA, Abad P, Rascovsky S et al (2014) Assessment of cardiac volumes using an isotropic whole-heart dual cardiac phase sequence in pediatric patients. J Magn Reson Imaging 39:708–716
Jaroni J, Meier R, Beer A et al (2013) Three-dimensional magnetic resonance imaging using single breath-hold k-t BLAST for assessment of global left ventricular functional parameters. Acad Radiol 20:987–994
van der Meulen P, Groen JP, Tinus AM et al (1988) Fast field echo imaging: an overview and contrast calculations. Magn Reson Imaging 6:355–368
Plein S, Bloomer TN, Ridgway JP et al (2001) Steady-state free precession MRI of the heart: comparison with segmented k-space gradient-echo imaging. J Magn Reson Imaging 14:230–236
Carr JC, Simonetti O, Bundy J et al (2001) Cine MR angiography of the heart with segmented true fast imaging with steady-state precession. Radiology 219:828–834
Mascarenhas NB, Muthupillai R, Cheong B et al (2006) Fast 3D cine steady-state free precession imaging with sensitivity encoding for assessment of left ventricular function in a single breath-hold. AJR Am J Roentgenol 187:1235–1239
Wech T, Pickl W, Tran-Gia J et al (2014) Whole-heart cine MRI in a single breath-hold – a compressed sensing accelerated 3D acquisition technique for assessment of cardiac function. Röfo 186:37–41
Sievers B, Schrader S, Rehwald W et al (2011) Left ventricular function assessment using a fast 3D gradient echo pulse sequence: comparison to standard multi-breath hold 2D steady state free precession imaging and accounting for papillary muscles and trabeculations. Acta Cardiol 66:349–357
Krishnamurthy R, Pednekar A, Atweh LA (2015) Clinical validation of free breathing respiratory triggered retrospectively cardiac gated cine steady-state free precession imaging in sedated children. J Cardiovasc Magn Reson 17:1–7
Pruessman KP, Weiger M, Boesiger P (2001) Sensitivity encoding cardiac MRI. J Cardiovasc Magn Reson 3:1–9
Tsao J, Boesiger P, Pruessmann KP (2003) k-t BLAST and k-t SENSE: dynamic MRI with high frame rate exploiting spatiotemporal correlations. Magn Reson Med 50:1031–1042
Barkhausen J, Ruehm SG, Goyen M et al (2001) MR evaluation of ventricular function: true fast imaging with steady-state precession versus fast low-angle shot cine MR imaging: feasibility study. Radiology 219:264–269
Hori Y, Yamada N, Higashi M et al (2003) Rapid evaluation of right and left ventricular function and mass using real-time true FISP cine MR imaging without breath-hold: comparison with segmented true-FISP cine MR with breath-hold. J Cardiovasc Magn Reson 5:439–450
Alfakih K, Pleine S, Thiele H et al (2003) Normal human left and right ventricular dimension for MRI as assessed by turbo gradient echo and steady-state free precession imaging sequences. J Magn Reson Imaging 17:323–329
Amano Y, Suzuki Y, van Cauteren M (2008) Evaluation of global cardiac functional parameters using single-breath-hold three-dimensional cine steady-state free precession MR imaging with two types of speed-up techniques: comparison with two-dimensional cine imaging. Comput Med Imaging Graph 32:61–66
Sardanelli F, Quarenghi M, Di Leo G et al (2008) Segmentation of cardiac cine MR images of left and right ventricles: interactive semiautomated methods and manual contouring by two readers with different education and experience. J Magn Reson Imaging 27:785–792
Reeder SB, Wintersperger BJ, Dietrich O et al (2005) Practical approaches to the evaluation of signal-to-noise ratio performance with parallel imaging: application with cardiac imaging and a 32-channel cardiac coil. Magn Reson Med 54:748–754
Wintersperger BJ, Reeder SB, Nikolaou K et al (2006) Cardiac CINE MR imaging with a 32-channel cardiac coil and parallel imaging: impact of acceleration factors on image quality and volumetric accuracy. J Magn Reson Imaging 23:222–227
Krishnamurthy R, Pednekar A, Atweh LA, Vogelius E, Chu ZD, Zhang W, Maskatia S, Masand P, Morris SA, Krishnamurthy R, Muthupillai R (2015) Clinical validation of free breathing respiratory triggered retrospectively cardiac gated cine balanced steady-state free precession cardiovascular magnetic resonance in sedated children. J Cardiovasc Magn Reson 17:(1). doi10.1186/s12968-014-0101-1
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
A. Pednekar, PhD, is an employee of Philips Healthcare. Authors report no other conflicts of interest.
Rights and permissions
About this article

Cite this article
Atweh, L.A., Dodd, N.A., Krishnamurthy, R. et al. Comparison of two single-breath-held 3-D acquisitions with multi-breath-held 2-D cine steady-state free precession MRI acquisition in children with single ventricles. Pediatr Radiol 46, 637–645 (2016). https://doi.org/10.1007/s00247-015-3531-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-015-3531-5