
Abstract
Background
Usually high-flow priapism is caused by perineal or penile blunt trauma with direct cavernosal artery injury and formation of an arterial-lacunar fistula. Rarely, cavernosal artery injury may result from penetrating trauma. Treatment of high-flow priapism is not considered an emergency because patients are at low risk for permanent complications. For this type of priapism there are several options for treatment including embolization or surgical ligation.
Objective
To describe the technique of superselective transcatheter embolization with the use of autologous blood clot and to discuss the long-term results.
Materials and methods
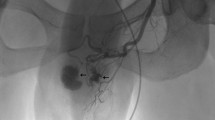
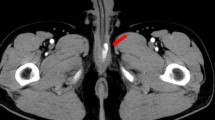
Seven children with a mean age of 10 years suffering from high-flow priapism were treated with superselective transcatheter embolization with autologous blood clot. In all cases, colour Doppler US was performed to demonstrate increased cavernous blood flow with definitive diagnosis established by superselective arteriography. After the angiographic diagnosis, superselective transcatheter embolization of the fistula with autologous blood clot was performed during the same session. The children were followed up on a monthly basis up to 1 year with clinical findings and penile colour Doppler US examinations. After 1 year, they were followed up annually with clinical assessment only. The mean follow-up period was 6.0 years.
Results
Following embolization complete detumescence was achieved in all but one child, who was treated with a second embolization 3 d after the initial session. In addition, for one child a second session of embolization was performed due to the recurrence of partial erection during the 1 week period after the initital embolization. In both cases, complete detumescence was achieved after the second embolization, and no recurrence of priapism was observed in the follow-up period.
Conclusion
Selective arterial embolization with autologous clot achieved treatment for high-flow priapism in this study with 100% occlusion rate with a maximum of two sessions and no signs of erectile dysfunction were observed in any of the children during long-term follow-up.



Similar content being viewed by others

References
Montague DK, Jarow J, Broderick GA et al (2003) Members of the erectile dysfunction guideline update panel; Americal Urological Association. American Urological Association guideline on the management of priapism. J Urol 170:1318–1324
Miller ST, Rao SP, Dunn EK et al (1995) Priapism in children with sickle cell disease. J Urol 154:844–847
Broderick GA, Gordon D, Hypolite J et al (1994) Anoxia and corporal smooth muscle dysfunction: a model for ischemic priapism. J Urol 151:259–262
Winter CC, McDowell G (1988) Experience with 105 patients with priapism: update review of all aspects. J Urol 140:980–983
Pryor J, Akkus E, Alter G et al (2004) Priapism. J Sex Med 1:116–120
Fratezi AC, Martins VM, Pereira Porta RM et al (2001) Endovascular therapy for priapism secondary to perineal trauma. J Trauma 50:581–584
Bastuba MD, Saenz de Tejada I, Dinlenc CZ et al (1994) Arterial priapism: diagnosis, treatment and long-term followup. J Urol 151:1231–1237
Leal J, Walker D, Egan EA (1978) Idiopathic priapism in the newborn. J Urol 120:376
Merlob P, Levine PM (1989) Incidence, possible causes and follow-up of idiopathic prolonged penile erection in the newborn. J Urol 141:1410–1412
Majeed S, Schor JA, Jacobson S et al (2000) Refractory priapism of unknown etiology in a pediatric patient. Pediatr Emerg Care 16:347–351
Witt MA, Goldstein I, Saenz de Tejada I et al (1990) Traumatic laceration of intracavernosal arteries: the pathophysiology of nonischemic, high flow, arterial priapism. J Urol 143:129–132
Miller SF, Chait PG, Burrows PE et al (1995) Posttraumatic arterial priapism in children: management with embolization. Radiology 196:59–62
Bertolotto M, Quaia E, Mucelli FP et al (2003) Color Doppler imaging of posttraumatic priapism before and after selective embolization. Radiographics 23:495–503
Kadioglu A, Sanli O, Celtik M et al (2006) Practical management of patients with priapism. EAU EBU Update Ser 4:150–160
Hatzichristou D, Salpiggidis G, Hatzimouratidis K et al (2002) Management strategy for arterial priapism: therapeutic dilemmas. J Urol 168:2074–2077
Ciampalini S, Savoca G, Buttazzi L et al (2002) High-flow priapism: treatment and long-term follow-up. Urology 59:110–113
Kuefer R, Bartsch G Jr, Herkommer K et al (2005) Changing diagnostic and therapeutic concepts in high flow priapism. Int J Impot Res 17:109–113
Persky L, Kursh E (1977) Post-traumatic priapism. J Urol 118:397–398
Wear JB Jr, Crummy AB, Munson BO (1977) A new approach to the treatment of priapism. J Urol 117:252–254
Numan F, Cantasdemir M, Ozbayrak M et al (2008) Posttraumatic nonischemic priapism treated with autologous blood clot embolization. J Sex Med 5:173–179
Callewaert P, Stockx L, Bogaert G et al (1998) Posttraumatic high-flow priapism in a 6-years old boy: management by percutaneous placement of bilateral vascular coils. Urology 52:134–137
Numan F, Cakirer S, Islak C et al (1996) Posttraumatic high-flow priapism treated by N-butyl– cyanoacrylate emblization. Cardiovasc Interv Radiol 19:278–280
O’Sullivan P, Browne R, McEniff N et al (2006) Treatment of “high-flow” priapism with superselective transcatheter embolization: a useful alternative to surgery. Cardiovasc Interv Radiol 29:198–201
Kress O, Heidenreich A, Klose KJ et al (2002) Superselective embolization with coils in high-flow priapism. Cardiovasc Interv Radiol 25:326–329
Hakim LS, Kulaksızoglu H, Mulligan S et al (1996) Evolving concepts in the diagnosis and treatment of arterial high-flow priapism. J Urol 155:541–548
Cakan M, Altu Gcaron U, Aldemir M (2006) Is the combination of superselective transcatheter autologous clot embolization and duplex sonography-guided compression therapy useful treatment option for the patients with high-flow priapism. Int J Impot Res 18:141–145
Ciampalini S, Savoca G, Buttazi L et al (2002) High–flow priapism treatment and follow up. Urology 59:110–113
Gandini R, Spinelli A, Konda D et al (2004) Superselective embolization in posttraumatic priapism with glubran 2 acrylic glue. Cardiovasc Interv Radiol 27:544–548
Park JK, Jeong YB, Han YM (2001) Recanalisation of embolised cavernosal artery: restoring potency in a patient with high-flow priapism. J Urol 165:2002–2003
Sandler G, Chennapragada SM, Soundappan SV et al (2008) Pediatric high-flow priapism and super-selective angiography-an Australian perspective. J Pediatr Surg 43:1898–1901
Towbin R, Hurh P, Baskin K et al (2007) Priapism in children: treatment with embolotherapy. Pediatr Radiol 37:483–487
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cantasdemir, M., Gulsen, F., Solak, S. et al. Posttraumatic high-flow priapism in children treated with autologous blood clot embolization: long-term results and review of the literature. Pediatr Radiol 41, 627–632 (2011). https://doi.org/10.1007/s00247-010-1912-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-010-1912-3