
Abstract
Summary
Early renal dysfunction is associated with a 38% increased fracture risk in individuals aged 65 years and older. In men but not women, early renal dysfunction is associated with decreased femoral neck bone mineral density (BMD) which can be partially explained by increased parathyroid hormone (PTH) concentrations.
Introduction
It is uncertain whether early renal dysfunction is associated with osteoporosis and increased fracture risk. The aim of this study was to determine the relationship of decreased renal function with BMD and fracture risk and the role of PTH therein.
Methods
We analyzed data of participants aged 65 years and older from the Longitudinal Aging Study Amsterdam. A 6-year fracture follow-up was obtained in 1477 participants. BMD was measured by dual-energy x-ray absorptiometry (n = 535) and vertebral fractures by lateral spinal radiograph (n = 527) in a subsample at baseline. Glomerular filtration rate (eGFR) was estimated according to the modification of diet in renal disease equation and assessed by the five stages of chronic kidney disease (CKD).
Results
In men and women, eGFR < 57 ml/min/1.73 m2 (lowest quartile) compared to eGFR > 74 ml/min/1.73 m2 (highest quartile) was associated with a 38% increase in fracture risk after adjustment for relevant confounders [hazard ratio (95%CI): 1.38 (1.17 to 1.61)]. Also, CKD stages 3a and 3b were associated to a 28 and 46% increase in fracture risk, respectively, as compared to CKD stages 1 and 2 together (eGFR > 60 ml/min/1.73 m2) after adjustment for confounders. Renal function was not associated with prevalent vertebral fractures. In men, but not women, lowest quartile of eGFR was related to lower femoral neck BMD as compared to the highest quartile eGFR [unstandardized B (95%CI) − 0.052 g/cm2 (− 0.098 to − 0.006)], after adjustment for relevant confounders. Further adjustment for PTH attenuated this relationship by 27%.
Conclusions
In men and women, early decreased renal function (eGFR < 60 ml/min/1.73 m2) was related to increased incident any fracture risk but not with increased prevalence of vertebral fractures. In men, but not women, early renal dysfunction was related to lower femoral neck BMD which could statistically be partially explained by increased PTH concentrations.
Similar content being viewed by others


Introduction
Renal function decreases with age. In health aging adults, a steady decline of GFR (averaging about 0.75–1.0 ml/min/1.73 m2/year) has been consistently observed in cross-sectional studies [1]. Thus, some degree of chronic kidney disease (CKD) is very common in the elderly. At least 20% of adults in the USA of 65 years or older have evidence of moderate to severe CKD as defined by an estimated glomerular filtration rate (eGFR) of 60 ml/min per 1.73 m2 or less [2]. The origin of age-related changes in the kidney or the so-called early renal dysfunction is thought to be rooted in the reduction in glomerular mass mainly due to glomerulosclerosis [1].
Data from epidemiological studies have yielded controversial results regarding the association of CKD with bone mineral density (BMD) and fracture risk. An increased risk of hip fractures has been reported in patients with moderate and severe CKD [3, 4]. CKD was associated with accelerated bone loss in Afro-Caribbean men [5]. However, in one study, a GFR lower than 60 ml/min was not associated with increased fracture risk [6]. Thus, the relationship of in particular early renal function loss with fracture risk in older individuals remains unclear.
Potential mechanisms can be hypothesized to contribute to such an increased fracture risk. Moderate renal dysfunction is associated with higher phosphate concentrations and raised circulating concentrations of parathyroid hormone (PTH) in association with mainly cortical bone loss. In addition, deficient 25-hydroxyvitamin D (25(OH)D) concentrations are common in these patients and aggravate secondary hyperparathyroidism [7]. Vitamin D deficiency and secondary hyperparathyroidism have detrimental effects on bone, and this may explain part of the relationship between decreased renal function, osteoporosis, and fracture risk. It is not known whether early renal dysfunction or the age-related impairment is associated with osteoporosis and increased fracture risk. With this study, we hypothesized that early renal dysfunction in older individuals is associated with higher fracture risk and lower BMD and part of these relationships may be explained by an increase in serum parathyroid hormone concentrations and increased bone turnover.
This study aimed to determine and quantify the relationship of early renal dysfunction with fracture risk and BMD in a population-based older cohort [8]. In addition, parathyroid hormone (PTH), bone turnover, and falls were studied as potential contributing mechanisms to these relationships.
Materials and methods
Subjects
The study was performed using data of the Longitudinal Aging Study Amsterdam (LASA), an ongoing multidisciplinary cohort study on predictors and consequences of changes in physical, cognitive, emotional, and social functioning in the aging population in The Netherlands [8]. A random age and sex-stratified sample was drawn from population registries of 11 municipalities in three different regions of The Netherlands. The LASA study is a representative sample of older Dutch men and women. In total, 3107 subjects participated in the baseline examination (1992–1993).
The present study included participants who were born in or before 1930 (aged 65 years and older as of January 1, 1996) and participated in a follow-up examination in 1995–1996. After a main interview and a medical interview at home (n = 1509), participants were invited to a hospital or healthcare center to obtain blood and urine samples (n = 1328). Valid serum concentrations of creatinine could be determined in 1327 samples. The number of participants with both information of fracture follow-up and creatinine concentration was 1318.
BMD measurements of the lumbar spine and hip were obtained in a subsample in the geographical area of Amsterdam and surrounding communities including 535 participants. In LASA, the hip scan was usually made on the left site of the body. The study sample consisted of 522 participants with BMD measurements of the hip. Additional valid spinal radiographs were obtained in 527 of these participants.
The Medical Ethics Committee of the VU University Medical Center approved the study. Informed consent was obtained from all respondents.
Biochemistry
Blood samples were obtained in the morning and immediately centrifuged and frozen. Participants were allowed to have tea and toast [9], but no dairy products. The participants also brought an overnight urine sample for analysis. The serum and urine samples were promptly stored at − 20 °C. Serum creatinine (Cr) was determined as routine measurement according to local laboratory (in Zwolle, Oss and VUMC) procedures in fresh blood.
The serum creatinine concentration was used to estimate glomerular filtration rate (eGFR) according to the modification of diet in renal disease (MDRD) equation and the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation [10, 11].
Serum 25-hydroxyvitamin D (25(OH)D) was determined according to a competitive protein-binding assay in 1997/1998 (Nichols Diagnostics, San Juan Capistrano, CA, USA). The interassay coefficient of variation (CV) was 10%. Serum parathyroid hormone (PTH) was measured by means of an immunoradiometric assay (Incstar Corp., Stillwater, MN, USA), with an interassay CV of 12%. As a marker of bone formation, serum osteocalcin (OC) was measured by an immunoradiometric assay (Biosource/Medgenix Diagnostics, Fleuris, Belgium) with an interassay CV of 8%. Urinary deoxypyridinoline (DPD) was measured by a competitive luminescence immunoassay (ACS180 System; Bayer Diagnostics, Mijdrecht, The Netherlands) with an interassay CV of 8%. Values were corrected for creatinine (Cr) concentration in the same urine sample. Urine DPD/Cr excretion was calculated as a marker of bone resorption. These analyses were performed at the Endocrine Laboratory of the VU University Medical Center.
Bone mineral density and body composition
The dual-energy x-ray absorptiometry scans were made at the department of Nuclear Medicine, using a Hologic QDR2000 scanner (Hologic Inc., Waltham, MA, USA). All BMD measurements were performed with the same DXA scanner.
The lumbar spine (L1-L4) and hip (femoral neck, trochanter, and total hip) were scanned at baseline and 3 years later. Body composition including fat mass, fat-free mass, bone area, and bone mineral content for the extremities was scanned at baseline. The amount of fat-free soft tissue (lean mass minus BMC) of the extremities was used as an indicator of skeletal muscle mass [12].
Fracture and fall assessment
Fractures were assessed using two different methods [13]. A fall and fracture calendar was used in the first 3 years (1995/96–1998/99). Participants were instructed to complete a set of questions regarding fractures every 3 months. In addition, fractures were assessed by an interview at the end of the 3-year period in the second period (1998/99–2001/02). The exact date of the fracture was asked and verified with the general practitioner or hospital records. More than 90% of the fractures included in the analyses could be verified. In case of individuals who dropped out or were deceased, the general practitioner was interviewed about potential fractures and the circumstances of the fractures. In the present study, “any fracture” was defined as any kind of fracture except for fractures in the hand/finger, foot/toe, and head/neck and traffic accidents.
Prevalent vertebral fractures were assessed on lateral radiographs. Lateral radiographs of the thoracic and lumbar spine (T4–L5) were made at the end of 1995 or in 1996. The presence and degree of prevalent vertebral deformity were assessed by a semiquantitative method (mild deformity, 20–25% reduction in anterior, central, or posterior vertebral height; moderate deformity, 25–40% reduction in vertebral height; severe deformity, > 40% reduction in vertebral height) according to the classification of Genant. In a random sample of 50 radiographs, the intra-observer agreement of this semiquantitative method was tested with weighted kappa-scores. Weighted kappa-scores for presence of deformity (y/n), severity, and number of deformities were 0.80, 0.75, and 0.63, respectively.
A 3-year fall follow-up was performed with the fall and fracture calendar starting at the end of the second medical interview (1995/1996). The respondents were asked to record fall events weekly until the third medical interview (1998/1999). A fall was defined as “an unintentional change in position resulting in coming to rest at a lower level or on the ground.”
Potential confounders
Age, sex, body mass index (BMI), alcohol, smoking, and chronic diseases were considered as potential confounders in the relationship of renal function with fracture risk and BMD. The serum PTH, serum OC, urinary DPD/Cr, serum 25(OH)D, and skeletal muscle mass were added separately to the statistical model because of a potential role in the causal pathway of decreased renal function and the outcomes studied.
Body weight (kg) was measured in subjects wearing underwear only, using a calibrated balance beam scale. Height (m) was measured using a stadiometer. Smoking (never, former, current smoker) and alcohol use (does not drink, light, moderate, and excessive drinking) were assessed by questionnaires. The alcohol consumption index developed by Garretsen was used to classify alcohol drinkers into four categories (very excessive, excessive, moderate, light) [14].
The presence of chronic diseases was assessed with a detailed self-report questionnaire that included seven major diseases groups, i.e., chronic obstructive pulmonary disease, cardiovascular disease, stroke, peripheral arterial disease, diabetes mellitus, cancer, and joint disorders (osteoarthritis/rheumatoid arthritis).
Statistical analyses
Baseline characteristics of the study population were presented as mean ± SD for continuous variables, median (interquartile range) for skewed variables, and percentages for categorical variables. Multiple linear regression analyses were performed to study associations of renal function with BMD. Conditions for linear regression analysis were checked by histograms and normal probability plots of the standardized residuals. Effect modification by age and sex in the relationship of renal function with fractures and BMD was studied. Effects of confounders were studied by adding these to the regression analyses. Associations of renal function with BMD changes were performed with baseline BMD as an additional confounder.
Effect modification was defined as statistically significant interaction (p < 0.10). Associations with fracture and fall risk were analyzed using Cox proportional hazards regression and associations with prevalent vertebral fractures with logistic regression. Linearity of potential confounders was checked by adding dummies to the model and by adding a quadratic term. Multi-collinearity was checked by calculating correlation coefficients between the independent variables.
Statistical significance was based on p < 0.05. IBM SPSS Statistics 20 (SPSS, Inc., Chicago, IL, USA) was used for statistical analyses.
Results
Participant characteristics
Table 1 presents the baseline characteristics of the study population. A total of 715 men and 762 women participated in the analyses for fracture outcome in the present study. More than 99% of the population was of Caucasian race. The number of participants with severe CKD (CKD stages 4 and 5) was 5 (1.0%) and 13 (1.0%) in the population available for BMD and fracture analyses, respectively. The number of participants with PTH ≥ 10 pmol/l was 10 (1.9%) and 21 (1.6%) in the population for BMD and fracture analysis, respectively. Of the population for BMD and fracture analysis, 267 (51.5%) and 632 (48.2%) had 25(OH)D concentrations < 50 nmol/l, respectively. PTH concentrations according to CKD stages were 3.0 ± 1.3, 3.3 ± 1.7, 3.9 ± 3.1, 6.0 ± 2.9, 11.8 ± 7.4, and 11.8 ± 8.9 pmol/l for stage 1 (n = 47), stage 2 (n = 737), stage 3a (n = 429), stage 3b (n = 110), stage 4 (n = 16), and stage 5 (n = 5), respectively. Concentrations of 25-hydroxyvitamin D according to CKD stages were 54 ± 24, 54 ± 24, 54 ± 24, 45 ± 23, 56 ± 24, and 28 ± 9 nmol/l for stage 1 (n = 47), stage 2 (n = 860), stage 3a (n = 327), stage 3b (n = 62), stage 4 (n = 9), and stage 5 (n = 3), respectively.
Associations of renal function with any fracture incidence
During 6-year follow-up, 132 out of 1477 participants (8.9%) experienced at least one fracture. Seventeen participants (1.2%) had 2 fractures, 3 participants (0.2%) had 3 fractures, and 1 participant had 4 fractures. The number of fractures (%) that occurred at specific sites was as follows: hip 37 (28%), wrist 33 (25%), vertebra 14 (11%), rib 14 (11%), humerus 10 (8%), fracture of lower extremity (not hip or ankle) 10 (8%), fracture of upper extremity (not wrist or humerus) 7 (5%), ankle 6 (5%), and pelvis 1 (1%). Of 108 of 132 fractures, the cause was registered. Of these, 61 (57%) were the consequence of a fall from less than standing height, and 9 (8%) resulted from a fall of more than standing height. Of 36 fractures (33%), the cause was registered as unknown.
In the present study, age and sex were not effect modifiers in the association of renal function with incidence of fractures or falls (p > 0.10). Therefore, all analyses with fracture or fall incidence as the outcome were performed and described in the total population. The association of renal function with fracture incidence is presented in Tables 2 and 3. The association between the continuous variables eGFR and fracture incidence did not fulfill the conditions for linear regression. Therefore, eGFR quartiles were used (Table 2), and eGFR was classified according to CKD stages 1 until 5 (Table 3).
The quartile group with the lowest eGFR(MDRD) (< 57 ml/min/1.73 m2) as compared to the highest eGFR(MDRD) (> 74 ml/min/1.73 m2) was characterized by an increased risk for fracture after correction for age and sex (Table 2; model 1). Adjustment for additional confounders (BMI, smoking, alcohol, number of chronic disease) and PTH did not influence this relationship (Table 2; models 2 and 3, respectively). In the adjusted model 2, the quartile group with the lowest eGFR(MDRD) quartile had a 38% increase in fracture risk as compared to the highest eGFR(MDRD) quartile. Compared to the highest quartile, the lowest quartile (lowest eGFR) was related to a 46% increase in fracture risk [HR = 1.46 (95%CI 1.23–1.73)] after addition of serum 25(OH)D and bone turnover markers (BTMs) serum OC and DPD/Cr ratio to model 2. Further adjustment of model 2 for skeletal muscle mass did not materially alter the relationship (n = 516).
The results of the analyses performed with eGFR(CKD-EPI) did not alter the conclusions drawn from the analyses with eGFR(MDRD).
Classification according to CKD stages based on MDRD resulted in a 28 and 46% increase in fracture risk for stages 3a and 3b, respectively, after adjustment for additional confounders (Table 3; model 2) as compared to stages 1 and 2 together (eGFR > 60 ml/min/1.73 m2). CKD stage 1 could not be used as a separate reference category because the number of fractures in this category was too small (n = 6). Stage 3a and stage 3b CKD were related to a 32 and 52% increase in fracture risk [HR = 1.32 (95%CI 1.15–1.50) and HR 1.52 (95%CI 1.16–2.00)], respectively, after further addition of serum 25(OH)D and BTMs serum OC and DPD/Cr ratio to model 2. Addition of PTH concentrations to the model did not influence the association between CKD stage and fracture risk (Table 3; model 3).
Associations of renal function with vertebral fracture prevalence
Of the 521 participants with vertebral fracture assessment, 245 (47%) had at least one vertebral fracture. Of the study population, 139 (27%) individuals had 1 vertebral fracture, 60 (12%) had 2 vertebral fractures, and 46 (9%) had 3 or more vertebral fractures. The number of participants with at least one vertebral fracture of moderate severity was 88 (17%), and the number with at least one severe vertebral fracture was 11 (2%).
The lowest quartile of eGFR (MDRD) was not related to a higher risk of prevalent vertebral fractures as compared to the highest quartile group after adjustment of potential confounders BMI, smoking, alcohol, and number of chronic disease [OR 0.74 (95%CI 0.45–1.22), n = 59/126 (47%) and n = 58/116 (50%), respectively]. In addition, CKD stages 3a and 3b (MDRD) were not associated with a higher risk of prevalent vertebral fractures as compared to the reference category, i.e., CKD stages 1 and 2 together [CKD stage 3a: n = 59/125 (47%), OR 0.86 (95%CI 0.56–1.32) and stage 3b: n = 10/24 (42%), OR 0.63 (0.53–1.24); stage CKD 1 and 2, 174/367 (47%)]. The number of vertebral fractures in stages 4 (n = 3) and 5 (n = 2) was too small to perform analyses.
Associations of renal function with fall incidence
In the present study, 800 out of 1435 participants (55.7%) experienced at least one fall. However, lowest quartile of eGFR (MDRD) was not associated with an increased risk of falls during 3-year follow-up as compared to the highest quartile (after adjustment for age, sex, BMI, smoking, alcohol, and number of chronic diseases, HR = 0.999 (0.995–1.002), p = 0.46).
Cross-sectional and longitudinal associations of renal function with BMD
The interaction analyses demonstrated that sex was an effect modifier in the association of eGFR with BMD (p < 0.10). Therefore, all analyses with BMD as the outcome were performed stratified for sex.
The association between the continuous variables eGFR and BMD did not fulfill the conditions for linear regression. Therefore, again, eGFR quartiles were used (Table 4) and eGFR was classified according to CKD stages 1 until 5.
In men, the femoral neck BMD range of the lowest eGFR(MDRD) quartile group was 0.360 to 1.090 g/cm2, and that of the highest eGFR(MDRD) quartile groups was 0.510 to 1.680 g/cm2.
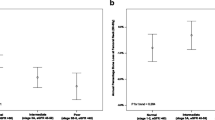
In men, the lowest eGFR(MDRD) quartile group (< 58 ml/min/1.73 m2) had significantly lower femoral neck BMD after adjustment for age, sex, BMI, smoking, alcohol, and number of chronic diseases, compared with the highest eGFR(MDRD) quartile group (> 74 ml/min/1.73 m2) (Table 3; models 1 and 2). This relationship was attenuated by 27% after further adjustment for PTH. Further adjustment of model 2 for serum 25(OH)D or serum OC and urinary DPD/Cr did not materially change the relationship [25(OH)D − 0.056 g/cm2 (95%CI − 0.103–− 0.009), p = 0.093; OC and DPD/Cr together − 0.042 g/cm2 (95%CI − 0.091–0.007), p = 0.090]. Also, adjustment for skeletal muscle mass did not materially affect the results [− 0.042 g/cm2 (95%CI − 0.091 to 0.007), p = 0.090].
The eGFR(CKD-EPI) range of quartiles was a little different from that of eGFR(MDRD), with 8–55 and 71–94 ml/min/1.73 m2 for the lowest and the highest quartile group, respectively. The results of the analyses using eGFR(CKD-EPI) were similar to the analyses using eGFR(MDRD), except for the third quartile of eGFR(CKD-EPI) which also was associated with a significantly lower femoral neck BMD as compared with the highest quartile [− 0.052 g/cm2 (95%CI − 0.097–− 0.008), p = 0.021]. The significance remained after further adjustment for PTH [− 0.049 g/cm2 (95%CI − 0.093–− 0.006), p = 0.027]. The second quartile did not reach significance. However, the estimates were very close to each other and results pointed in the same direction.
Classification according to stages of CKD resulted in lower, although not significantly, femoral neck BMD in men with CKD stage 3b [BMD 0.710 ± 0.145 g/cm2; − 0.042 g/cm2 (95%CI − 0.121–0.037), n = 11] and no difference with men with stage 3a [BMD 0.742 ± 0.131 g/cm2; − 0.007 g/cm2 [95%CI − 0.047–0.033], n = 54] as compared to the reference category consisting of stages 1 and 2 (BMD 0.747 ± 0.138 g/cm2, n = 188) after adjustment for additional confounders. The number of participants with CKD stages 4 (n = 3) and 5 (n = 2) was too small to perform an analyses on BMD outcomes.
In men, decreased renal function was not associated with baseline total hip BMD or lumbar spine BMD. In women, there were no associations between eGFR and BMD at any site.
Longitudinally, BMD change in 3 years was not different between eGFR quartile groups for any site in men and women.
Discussion
The principal findings of the present study are that in both older men and women, early decreased renal function (eGFR < 60 ml/min/1.73 m2) was related to increased incident fracture risk but not with increased prevalence of vertebral fractures or falls. In addition, decreased renal function was related to lower femoral neck BMD in men but not women. In men, this relationship could statistically be partly explained by higher PTH concentrations.
As for whether early renal dysfunction is associated with increased fracture risk in the general population, data from previous studies have yielded controversial results. Most studies on the association of eGFR and fractures studied hip fracture, vertebral fracture, or osteoporotic fracture incidence in selected populations with CKD, especially end-stage CKD. To our knowledge, no previous study selected any fracture as outcome in a population-based older cohort population. A community-based cohort of 1.8 million Canadian adults suggested that reduced eGFR (< 60 ml/min per 1.73 m2) was not associated with increased rates of incident hip, wrist, and vertebral fractures compared with normal renal function [6]. That study, however, had the limitation that the outcomes were based on coding of administrative data to identify fractures and defined comorbidities, which may have resulted in potential misclassification. Also, there was selection bias of participants with a measurement of creatinine concentration because the participants were identified from community-dwelling adults aged ≥ 18 years who had at least one outpatient serum creatinine measurement, on indication. In contrast, we examined fracture incidence using reliable data on fractures (fracture calendar, questions regarding fractures, and data verification through the general practitioner or hospital reports). Also, our random age and sex-stratified study sample was population-based.
End-stage CKD has been associated with a fourfold increased risk of osteoporotic fracture, even in young adults [15]. In our study, fracture risk increases as renal dysfunction worsens in a graded manner. This was also shown in a cohort study of 679,114 adults using healthcare databases from Ontario (Canada). In that study, the 3-year cumulative incidence of hip, forearm, pelvis, or proximal humerus fracture increased in a graded manner in adults with lower levels of eGFR [16]. Also, another study confirmed the association between mild to moderate reductions (eGFR 45–59 ml/min per 1.73 m2) in renal function and increased risk of hip fracture independently from traditional risk factors including age, body weight, and bone density [4]. The analysis of NHANES III data even suggested that this association between decreased renal function and higher fracture risk in CKD was stronger than many conventional risk factors for fracture, including BMD, sex, race, and age [17]. Our finding of an absent relationship between renal function and vertebral fractures is in agreement with a prospective study that could not identify an increased incident fracture risk [4]. However, a Japanese study did find increased vertebral fracture incidence related to renal function, although they focused on stage 2 as compared to stage 1 CKD because they had a low number of participants with CKD stage 3 and higher [18].
In our study, the association between decreased eGFR and femoral neck BMD is gender-specific. The reason of this gender-specific association is still unknown. It may be partially explained by the differences in peak bone mass and bone loss rates between sexes, which results in lower BMD in older women than elderly men. In older women, therefore, it may be more unlikely for BMD to further decrease as a consequence of the additional effect of mildly decreased eGFR. Also, in older women, other factors that determine BMD such as vitamin D deficiency may play a more important role than mildly decreased eGFR. From the controversial results of different studies, it is not difficult to understand that the mechanism behind the association between decreased eGFR and BMD/fracture risk is complicated. Reasons are multifactorial and include CKD mineral and bone disorder (CKD-MBD), i.e., abnormalities in phosphorous, calcium, parathyroid hormone, or vitamin D metabolism, and muscle loss [19, 20]. In large population-based older cohorts, common underlying risk factors in those with mild to moderate reduced eGFR are more usual than a unique pathophysiology as seen in patients with ESRD [6]. Loss of skeletal muscle (due to CKD and its comorbid conditions) increases risk of falls and frailty and in turn leads to more fractures [21]. Also, vitamin D deficiency is common in the general older population and also in those with mildly impaired renal function and may contribute to fall and fracture risk [22]. In our study, we could not explain the increased fracture risk by increased fall risk or decreased 25(OH)D concentrations or muscle mass. Whatever the underlying mechanism, the increased risk is important for fracture risk estimation in the general population. Fracture risk evaluation should take renal function into account, and even mildly decreased renal function should be included in guidelines.
In renal disease, decreasing GFR is associated with increased PTH secretion [23]. Elevated PTH is strongly associated with cortical bone loss [24]. However, results of the relationship between PTH and BMD are conflicting [25, 26]. Studies on the association between PTH and fracture risk in patients with end-stage CKD also showed contradictory results [27,28,29]. One reason for the different conclusions is that serum PTH has a short half-life and depends on calcium intake. In our study, the association between lower eGFR and lower femoral neck BMD in men is partly determined by PTH. PTH specifically influences cortical bone remodeling and therefore may explain its impact on the relationship between eGFR and specifically femoral neck BMD. The 2017 Updated KDIGO CKD-MBD Guideline encourages the continued use of PTH trends to identify different types of bone involvement in CKD-MBD [30].
The strengths of our study are its prospective cohort design including men and women, being a representative well-phenotyped sample of the older Dutch population, and the combination of bone density measurements at various sites with a reliable assessment of falls and fractures. The sufficient sample size enabled us to test possible confounders and effect modifiers. So far, few population-based prospective studies in older individuals have investigated the association of renal dysfunction with risk of any fracture (instead of hip, spine, or osteoporotic fracture). This study also has some limitations. First, renal function was assessed only at one time point. In older individuals, creatinine concentrations can be temporarily elevated by a wide variety of causes without true renal function loss. Also, the absence of analyses of longitudinal data of renal function and other biochemical parameters such as PTH limited the possibility to study of effects of longitudinal changes. Second, a direct measure of GFR was not available; we used both MDRD and CKD-EPI equation to estimate GFR. The reason for also using the MDRD equation is to allow comparison with previous results. The equations are creatinine-dependent, while serum creatinine alone is a less reliable measure of renal function in older persons, because of a decline in muscle mass and alteration in creatinine metabolism with age [31]. Third, the population-based recruitment yielded low numbers with CKD stages 4 and 5 and did not allow us to study effects of moderate to severe CKD separately. Fourth, BMD, vertebral fracture prevalence, and skeletal muscle mass were assessed only in a subsample of the total population which limits the power to find effects. Fifth, the available BTM concentrations, OC, and DPD/Cr ratio are affected by renal clearance [32]. The use of other BTMs, which are not dependent on renal function such as TRAP-5b and P1NP, may have led to different results. Sixth, we did not adjust for competing risks in the analyses. Participants with CKD have a higher risk of death than participants without CKD and therefore are less likely to reach the primary end point, i.e., a fracture, during follow-up. However, if anything, this competing risk may have resulted in an underestimation of the true effect of eGFR on fracture risk. Finally, the cohort analyzed in this study was recruited in 1992 and the data originate from the measurement cycle in 1995 which may have contributed, for example, to the application of analytical methods that are currently no longer used.
In the future, one may consider cystatin C as a more valid marker for renal function estimation to overcome the limitations of serum creatinine [33]. Deterioration of renal function assessed by CKD-EPI-Cys better correlates with osteopenia than calculated eGFR using creatinine-based methods in CKD patients [34]. The CKD-EPI-Cys formula might be a useful tool to assess skeletal-related event risks. Given the adverse health consequences and economic burden associated with fractures [35, 36], identifying the cut-off of eGFR for increased risk of fractures would be important. The gender-specific effect of PTH on the relationship between eGFR and BMD needs to be confirmed.
In conclusion, in a population-based older cohort, we examined the association of decreased eGFR with BMD and fracture risk. Quite modest declines in renal function (eGFR < 60 ml/min/1.73 m2) were associated with increased fracture risk in both men and women. Decreased eGFR was accompanied by decreased BMD only in men and only in the femoral neck, and parathyroid hormone was identified as a potential partial mediator in this relationship. This latter finding suggests the importance of other factors than BMD in fracture risk such as impaired bone quality. Nevertheless, fracture risk evaluation should take renal function into account and even mildly decreased renal function should be included in guidelines and fracture prediction tools as a risk factor for future fractures.
Abbreviations
- BMD:
-
Bone mineral density
- PTH:
-
Parathyroid hormone
- LASA:
-
Longitudinal Aging Study Amsterdam
- eGFR:
-
Estimate glomerular filtration rate
- MDRD:
-
Modification of diet in renal disease
- CKD-EPI:
-
Chronic Kidney Disease Epidemiology Collaboration
- CKD:
-
Chronic kidney disease
- 25(OH)D:
-
25-Hydoxyvitamin D
- Cr:
-
Creatinine
- OC:
-
Osteocalcin
- DPD:
-
Deoxypyridinoline
- BMI:
-
Body mass index
- BTMs:
-
Bone turnover markers
References
Glassock RJ, Denic A, Rule AD (2017) The conundrums of chronic kidney disease and aging. J Nephrol 30:477–483
Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS (2003) Prevalence of chronic kidney disease and decreased kidney function in the adult US population: Third National Health and Nutrition Examination Survey. Am J Kidney Dis 41:1–12
Alem AM, Sherrard DJ, Gillen DL, Weiss NS, Beresford SA, Heckberd SR, Wong C, Stehman-Breen C (2000) Increased risk of hip fracture among patients with end-stage renal disease. Kidney Int 58:396–399
Ensrud KE, Lui L-Y, Taylor BC, Ishani A, Shlipak MG, Stone KL, Cauley JA, Jamal SA, Antoniucci DM, Cummings SR, Osteoporotic Fractures Research Group (2007) Renal function and risk of hip and vertebral fractures in older women. Arch Intern Med 167:133–139
Kuipers AL, Egwuogu H, Evans RW, Patrick AL, Youk A, Bunker CH, Zmuda JM (2015) Renal function and bone loss in a cohort of Afro-Caribbean men. J Bone Miner Res Off J Am Soc Bone Miner Res 30:2215–2220
Elliott MJ, James MT, Quinn RR, Ravani P, Tonelli M, Palacios-Derflingher L, Tan Z, Manns BJ, Kline GA, Ronksley PE, Hemmelgarn BR (2013) Estimated GFR and fracture risk: a population-based study. Clin J Am Soc Nephrol: CJASN 8:1367–1376
Taal MW, Thurston V, McIntyre NJ, Fluck RJ, McIntyre CW (2014) The impact of vitamin D status on the relative increase in fibroblast growth factor 23 and parathyroid hormone in chronic kidney disease. Kidney Int 86:407–413
Huisman M, Poppelaars J, Mvd H, Beekman AT, Brug J, TGv T, Deeg DJ (2011) Cohort profile: the Longitudinal Aging Study Amsterdam. Int J Epidemiol 40:868–876
Kuchuk NO, Pluijm SMF, Schoor NMV, Looman CWN, Smit JH, Lips P (2009) Relationships of serum 25-hydroxyvitamin D to bone mineral density and serum parathyroid hormone and markers of bone turnover in older persons. J Clin Endocrinol Metab 94:1244–1250
Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D (1999) A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med 130:461–470
Levey AS, Stevens LA, Schmid CH, Zhang Y(L), Castro AF III, Feldman HI, Kusek JW, Eggers P, van Lente F, Greene T, Coresh J, for the CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) (2009) A new equation to estimate glomerular filtration rate. Ann Intern Med 150:604–612
Visser M, Deeg DJH, Lips P, Harris TB, Bouter LM (2000) Skeletal muscle mass and muscle strength in relation to lower-extremity performance in older men and women. J Am Geriatr Soc 48:381–386
Schoor NMV, Visser M, Pluijm SMF, Kuchuk N, Smit JH, Lips P (2008) Vitamin D deficiency as a risk factor for osteoporotic fractures. Bone 42:260–266
van Balkom AJLM, Beekman ATF, de Beurs E, Deeg DJH, van Dyck R, van Tilburg W (2000) Comorbidity of the anxiety disorders in a community-based older population in The Netherlands. Acta Psychiatr Scand 101:37–45
Ball AM, Gillen DL, Sherrard D, Weiss NS, Emerson SS, Seliger SL, Kestenbaum BR, Stehman-Breen C (2002) Risk of hip fracture among dialysis and renal transplant recipients. JAMA 288:3014–3018
Naylor KL, McArthur E, Leslie WD, Fraser LA, Jamal SA, Cadarette SM, Pouget JG, Lok CE, Hodsman AB, Adachi JD, Garg AX (2014) The three-year incidence of fracture in chronic kidney disease. Kidney Int 86:810–818
Nickolas TL, McMahon DJ, Shane E (2006) Relationship between moderate to severe kidney disease and hip fracture in the United States. J Am Soc Nephrol 17:3223–3232
Kaji H, Yamauchi M, Yamaguchi T, Shigematsu T, Sugimoto T (2010) Mild renal dysfunction is a risk factor for a decrease in bone mineral density and vertebral fractures in Japanese postmenopausal women. J Clin Endocrinol Metab 95:4635–4642
Group. KDIGOKC-MW (2009) KDIGO clinical practice guidelines for the prevention, diagnosis, evaluation, and treatment of chronic kidney disease-mineral and bone disorder (CKD-MBD). Kidney Int 76:S1–S130
West SL, Jamal SA, Lok CE (2012) Tests of neuromuscular function are associated with fractures in patients with chronic kidney disease. Nephrol Dial Transplant 27:2384–2388
Lopes AA, Lantz B, Morgenstern H, Wang M, Bieber BA, Gillespie BW, Li Y, Painter P, Jacobson SH, Rayner HC, Mapes DL, Vanholder RC, Hasegawa T, Robinson BM, Pisoni RL (2014) Associations of self-reported physical activity types and levels with quality of life, depression symptoms, and mortality in hemodialysis patients: the DOPPS. Clin J Am Soc Nephrol: CJASN 9:1702–1712
Lee Y-h, Kim JE, Roh YH, Choi HR, Rhee Y, Kang DR, Lim S-K (2014) The combination of vitamin D deficiency and mild to moderate chronic kidney disease is associated with low bone mineral density and deteriorated femoral microarchitecture: results from the KNHANES 2008-2011. J Clin Endocrinol Metab 99:3879–3888
Levin A, Bakris G, Molitch M, Smulders M, Tian J, Williams L, Andress D (2007) Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: results of the study to evaluate early kidney disease. Kidney Int 71:31–38
Duan Y, Luca VD, Seeman E (1999) Parathyroid hormone deficiency and excess: similar effects on trabecular bone but differing effects on cortical bone. J Clin Endocrinol Metab 84:718–722
Jadoul M, Albert J, Akiba T, Akizawa T, Arab L, Bragg-Gresham J, Mason N, Prutz K-G, Young E, Pisoni R (2006) Incidence and risk factors for hip or other bone fractures among hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study. Kidney Int 70:1358–1366
Fidan N, Inci A, Coban M, Ulman C, Kursat S (2016) Bone mineral density and biochemical markers of bone metabolism in predialysis patients with chronic kidney disease. J Investig Med 64:861–866
Fishbane S, Hazzan AD, Jhaveri KD, Ma L, Jr EL (2016) Bone parameters and risk of hip and femur fractures in patients on hemodialysis. Clin J Am Soc Nephrol: CJASN 11:1063–1072
Fuller DS, Pisoni RL, Bieber BA, Gillespie BW, Robinson BM (2013) The DOPPS Practice Monitor for US dialysis care: trends through December 2011. Am J Kidney Dis 61:342–346
Iimori S, Mori Y, Akita W, Kuyama T, Takada S, Asai T, Kuwahara M, Sasaki S, Tsukamoto Y (2012) Diagnostic usefulness of bone mineral density and biochemical markers of bone turnover in predicting fracture in CKD stage 5D patients—a single-center cohort study. Nephrol Dial Transplant 27:345–351
Ketteler M, Block GA, Evenepoel P, Fukagawa M, Herzog CA, McCann L, Moe SM, Shroff R, Tonelli MA, Toussaint ND, Vervloet MG, Leonard MB (2017) Executive summary of the 2017 KDIGO Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Guideline Update: what’s changed and why it matters. Kidney Int 92:26–36
Weber JA, APv Z (1991) Interferences in current methods for measurements of creatinine. Clin Chem 37:695–700
Vervloet MG, Brandenburg VM, working C-M, ERA-EDTA go (2017) Circulating markers of bone turnover. Journal of Nephrology 1–8
Inker LA, Schmid CH, Tighiouart H, Eckfeldt JH, Feldman HI, Greene T, Kusek JW, Manzi J, van Lente F, Zhang YL, Coresh J, Levey AS, CKD-EPI Investigators (2012) Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med 367:20–29
Kwon YE, Lee MJ, Park KS, Han SH, Yoo TH, Oh KH, Lee J, Lee KB, Chung W, Kim YH, Ahn C, Choi KH (2017) Cystatin C is better than serum creatinine for estimating glomerular filtration rate to detect osteopenia in chronic kidney disease patients. Yonsei Med J 58:380–387
Schumock GT, Sprague SM (2007) Clinical and economic burden of fractures in patients with renal osteodystrophy. Clin Nephrol 67:201–208
Doan QV, Gleeson M, Kim J, Borker R, Griffiths R, Dubois RW (2007) Economic burden of cardiovascular events and fractures among patients with end-stage renal disease. Curr Med Res Opin 23:1561–1569
Acknowledgments
This study is based on data collected in the context of the Longitudinal Aging Study Amsterdam (LASA), which is largely funded by the Ministry of Health, Welfare, and Sports of The Netherlands. We specially acknowledge Jonathan Reeve for his contribution to the manuscript. We acknowledge The Netherlands Organisation for Health Research and Development for providing a visitor’s grant (040.11.570) which allowed Dr. Hailing Chen to perform a fellowship at the Department of Internal Medicine, Endocrine section, at the VU University Medical Center in Amsterdam.
Funding
This study was funded by a visitor grant of the Dutch Organization for Scientific Research (Nederlandse Organisatie voor Wetenschappelijk Onderzoek, NWO) to Dr. Hailing Chen.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The Medical Ethics Committee of the VU University Medical Center approved the study.
Conflicts of interest
Dr. Lips gave advice to Friesland-Campina. RT de Jongh received consultancy fees or participated in the advisory board of Shire, Amgen, and Lilly. None of the other authors have any conflicts of interest.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Chen, H., Lips, P., Vervloet, M.G. et al. Association of renal function with bone mineral density and fracture risk in the Longitudinal Aging Study Amsterdam. Osteoporos Int 29, 2129–2138 (2018). https://doi.org/10.1007/s00198-018-4592-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-018-4592-8