
Abstract
Purpose
Early clinical examination combined with MRI allows accurate diagnosis of syndesmosis instability after a high ankle sprain. However, patients often present late. The aims of the current study were to describe MRI characteristics associated with syndesmosis instability and to test the hypothesis that MRI patterns would differ according to time from injury.
Methods
Over a 5-year period, 164 consecutive patients who had arthroscopically proven syndesmosis instability requiring fixation were retrospectively studied. Patients with distal fibula fractures were not included. Injuries were classified as acute in 108 patients (< 6 weeks), intermediate in 32 (6–12 weeks) and chronic in 24 patients (> 12 weeks).
Results
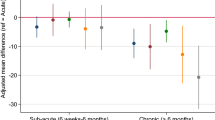
Posterior malleolus bone oedema was noted in 65 (60.2%), and posterior malleolus fracture in 17 (15.7%) of acute patients, respectively, which did not significantly differ over time. According to MRI, reported rates of posterior syndesmosis disruption significantly differed over time, observed in 101 (93.5%), 28 (87.5%) and 13 (54.2%) of acute, intermediate and chronic patients, respectively (p < 0.001). Apparent rates of PITFL injury significantly reduced with time (p < 0.001).
Conclusions
MRI detected a posterior syndesmosis injury in 93.5% of patients acutely but became less reliable with time. The clinical relevance of this study is that posterior malleolus bone oedema may be the only marker of a complete syndesmosis injury and can help clinically identify those injuries which require arthroscopic assessment for instability. If suspicious of a high ankle sprain, we advocate early MRI assessment to help determine stable versus unstable injuries as MRI becomes less reliable after 12 weeks.
Level of evidence
III.






Similar content being viewed by others


Abbreviations
- MRI:
-
Magnetic resonance imaging
- AITFL:
-
Anterior inferior tibio-fibular ligament
- IOL:
-
Intra-osseous ligament
- PITFL:
-
Posterior inferior tibio-fibular ligament
- IQR:
-
Interquartile range
- ATFL:
-
Anterior talo-fibular ligament
- CFL:
-
Calcaneo-fibular ligament
- PTFL:
-
Posterior talo-fibular ligament
References
Beumer A, Heijboer RP, Fontijne WP, Swierstra BA (2000) Late reconstruction of the anterior distal tibiofibular syndesmosis: good outcome in 9 patients. Acta Orthop Scand 71(5):519–521
Beumer A, van Hemert WL, Niesing R, Entius CA, Ginai AZ, Mulder PG, Swierstra BA (2004) Radiographic measurement of the distal tibiofibular syndesmosis has limited use. Clin Orthop Relat Res 423:227–234
Bonin JG (1950) Injuries to the ankle. William Heinemann Medical Books Ltd, London, pp 248–260
Boytim MJ, Fischer DA, Neumann L (1991) Syndesmotic ankle sprains. Am J Sports Med 19:294–298
Brown KW, Morrison WE, Schwetzer ME, Parellada A, Nothnagel H (2004) MRI findings associated with distal tibiofibular syndesmosis injuries. Am J Roentgenol 182:131–136
Calder JD, Bamford R, Petrie A, McCollum GA (2016) Stable versus unstable grade II high ankle sprains: a prospective study predicting the need for surgical stabilization and time to return to sports. Arthroscopy 32(4):634–642
Calder J, Mitchell A, Lomax A, Ballal MS, Grice J, van Dijk CN, Lee J (2017) The broken “ring of fire”: a new radiological sign as predictor of syndesmosis injury? Orthop J Sports Med 5(3):2325967117695064
Clanton TO, Ho CP, Williams BT, Surowiec RK, Gatlin CC, Haytmanek CT, LaPrade RF (2016) Magnetic resonance imaging characterization of individual ankle syndesmosis structures in asymptomatic and surgically treated cohorts. Knee Surg Sports Traumatol Arthrosc 24(7):2089–2102
Clanton TO, Williams BT, Backus JD, Dornan GJ, Liechti DJ, Whitlow SR, Saroki AJ, Turnbull TL, LaPrade RF (2017) Biomechanical analysis of the individual ligament contributions to syndesmotic stability. Foot Ankle Int 38(1):66–75
Forschner PF, Beitzel K, Imhoff AB, Buchmann S, Feuerriegel G, Hofmann F et al (2017) Five-year outcomes after treatment for acute instability of the tibiofibular syndesmosis using a suture-button fixation system. Orthop J Sports Med 5(4):2325967117702854
Gardner MJ, Brodsky A, Briggs SM, Nielson JH, Lorich DG (2006) Fixation of posterior malleolar fractures provides greater syndesmotic stability. Clin Orthop Relat Res 447:165–171
Gerber JP, Williams GN, Scoville CR, Arciero RA, Taylor DC (1998) Persistent disability associated with ankle sprains: a prospective examination of an athletic population. Foot Ankle Int 19(10):653–660
Han SH, Lee JW, Kim S, Suh JS, Choi YR (2007) Chronic tibiofibular syndesmosis injury: the diagnostic efficiency of magnetic resonance imaging and comparative analysis of operative treatment. Foot Ankle Int 28(3):336–342
Harper MC (2001) Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int 22(1):15–18
Hermans JJ, Ginai AZ, Wentink N, Hop WC, Beumer A (2011) The additional value of an oblique image plane for MRI of the anterior and posterior distal tibiofibular syndesmosis. Skelet Radiol 40(1):75–83
Hopkinson WJ, St Peirre P, Ryan JB, Wheeler JH (1990) Syndesmosis sprains of the ankle. Foot Ankle 10(6):325–330
Howard DR, Rubin DA, Hillen TJ, Nissman DB, Lomax J et al (2012) Magnetic resonance imaging as a predictor of return to play following syndesmosis (high) ankle sprains in professional football players. Sports Health 4(6):535–543
Lubberts B, Guss D, Vopat BG, Johnson AH, van Dijk CN, Lee H, DiGiovanni CW (2018) The arthroscopic syndesmotic assessment tool can differentiate between stable and unstable ankle syndesmoses. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-018-5229-3
McCollum GA, van den Bekerom MP, Kerkhoffs GM, Calder JD, van Dijk CN (2013) Syndesmosis and deltoid ligament injuries in the athlete. Knee Surg Sports Traumatol Arthrosc 21(6):1328–1337
Muhl C, Frank LR, Rand T (1998) Tibiofibular syndesmosis: high resolution MRI using a local gradient coil. J Comput Assist Tomogr 22:938–944
Nielson JH, Gardner MJ, Peterson MG, Sallis JG, Potter HG, Helfet DL, Lorich DG (2005) Radiographic measurements do not predict syndesmotic injury in ankle fractures: an MRI study. Clin Orthop Relat Res 436:216–221
Nussbaum ED, Hosea TM, Sieler SD, Incremona BR, Kessler DE (2001) Prospective evaluation of syndesmotic ankle sprains without diastasis. Am J Sports Med 29(1):31–35
Oae K, Takao M, Naito K, Uchio Y, Kono T, Ishida J, Ochi M (2003) Injury of the tibiofibular syndesmosis: value of MR imaging for diagnosis. Radiology 227(1):155–161
Ogilvie-Harris DJ, Reed SC, Hedman TP (1994) Disruption of the ankle syndesmosis: biomechanical study of the ligamentous restraints. Arthroscopy 10(5):558–560
Rammelt S, Zwipp H, Grass R (2008) Injuries to the distal tibiofibular syndesmosis: an evidence-based approach to acute and chronic lesions. Foot Ankle Clin 13(4):611–633
Rios AM, Rosenberg ZS, Bencardino JT, Rodrigo SP, Theran SG (2011) Bone marrow edema patterns in the ankle and hindfoot: distinguishing MRI features. Am J Roentgenol 197(4):W720–W729
Sikka RS, Fetzer GB, Sugarman E, Wright RW, Fritts H, Boyd JL, Fischer DA (2012) Correlating MRI findings with disability in syndesmotic sprains of NFL players. Foot Ankle Int 33(5):371–378
Sman AD, Hiller CE, Rae K, Linklater J, Black DA, Nicholson LL, Burns J, Refshauge KM (2015) Diagnostic accuracy of clinical tests for ankle syndesmosis injury. Br J Sports Med 49(5):323–329
Sman AD, Hiller CE, Refshauge KM (2013) Diagnostic accuracy of clinical tests for diagnosis of ankle syndesmosis injury: a systematic review. Br J Sports Med 47(10):620–628
Takao M, Ochi M, Oae K, Naito K, Uchio Y (2003) Diagnosis of a tear of the tibiofibular syndesmosis. The role of arthroscopy of the ankle. J Bone Jt Surg Br 85(3):324–329
Takao M, Ochi M, Naito K, Iwata A, Kawasaki K, Tobita M, Miyamoto W, Oae K (2001) Arthroscopic diagnosis of tibiofibular syndesmosis disruption. Arthroscopy 17(8):836–843
Taylor DC, Englehardt DL, Bassett FH (1992) Syndesmosis sprains of the ankle: the influence of heterotopic ossification. Am J Sports Med 20:146–150
Turky M, Menon KV, Saeed K (2018) Arthroscopic grading of injuries of the inferior tibiofibular syndesmosis. J Foot Ankle Surg 57(6):1125–1129
Van den Bekerom MP, Raven EE (2007) The distal fascicle of the anterior inferior tibiofibular ligament as a cause of tibiotalar impingement syndrome: a current concepts review. Knee Surg Sports Traumatol Arthrosc 15:465–471
van Dijk CN, Longo UQ, Loppini M, Florio P, Maltese L, Ciuffreda M, Denaro V (2016) Classification and diagnosis of acute isolated syndesmotic injuries: ESSKA-AFAS consensus guidelines. Knee Surg Sports Traumatol Arthrosc 24(4):1200–1216
van Dijk CN, Longo UQ, Loppini M, Florio P, Maltese L, Ciuffreda M, Denaro V (2016) Conservative and surgical management of acute isolated syndesmotic injuries: ESSKA-AFAS consensus guidelines. Knee Surg Sports Traumatol Arthrosc 24(4):1217–1227
Warner SJ, Garner MR, Schottel PC, Hinds RM, Loftus ML, Lorich DG (2015) Analysis of PITFL injuries in rotationally unstable ankle fractures. Foot Ankle Int 36(4):377–382
Whiteside LA, Reynolds FC, Ellsasser JC (1978) Tibiofibular synostosis and recurrent ankle sprains in high performance athletes. Am J Sports Med 6(4):204–208
Wright RW, Barile RJ, van den Bekerom MP, Raven EE (2007) The distal fascicle of the anterior inferior tibiofibular ligament as a cause of tibiotalar impingement syndrome: a current concepts review. Knee Surg Sports Traumatol Arthrosc 15(4):465–471
Acknowledgements
We would like to thank Satomi Okana for assisting in the data analysis, and Wesley Medical Research for funding costs towards statistical support.
Funding
Funding was provided by Wesley Medical Research.
Author information
Authors and Affiliations
Contributions
MR carried out data collection and writing of manuscript. DM carried out the ethics application, data collection and writing of manuscript. EB participated in study design, performed data analysis and contributed to writing of manuscript. BF conceived the study, participated in the study design and writing of manuscript. ML conceived the study, participated in the study design and writing of manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Ethics approval was obtained from the Uniting Health Care, Wesley Hospital, Ethics and 105 Review committee, approval number 2017.22.236.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Randell, M., Marsland, D., Ballard, E. et al. MRI for high ankle sprains with an unstable syndesmosis: posterior malleolus bone oedema is common and time to scan matters. Knee Surg Sports Traumatol Arthrosc 27, 2890–2897 (2019). https://doi.org/10.1007/s00167-019-05581-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-019-05581-5