
Abstract
Type 1 diabetes is an autoimmune disease caused by T cell-mediated destruction of pancreatic insulin-producing beta cells. The epitopes recognised by pathogenic T cells in human type 1 diabetes are poorly defined; however, a growing body of evidence suggests that T cell responses against neoepitopes contribute to beta cell destruction in type 1 diabetes. Neoepitopes are formed when self-proteins undergo post-translational modification to create a new epitope that is recognised by T- or B cells. Here we review the role of human T cell responses against neoepitopes in the immune pathogenesis of type 1 diabetes. Specifically, we review the different approaches to identifying neoepitopes relevant to human type 1 diabetes and outline several advances in this field that have occurred over the past few years. We also discuss the application of neoepitopes to the development of antigen-specific therapies for type 1 diabetes and the unresolved challenges that need to be overcome before the full repertoire of neoepitopes recognised by pathogenic human T cells in type 1 diabetes can be determined. This information may then be used to develop antigen-specific therapies for type 1 diabetes and assays to monitor changes in pathogenic, beta cell-specific T cell responses.
Similar content being viewed by others

Type 1 diabetes
Type 1 diabetes is an autoimmune disease caused by the autoimmune destruction of pancreatic insulin-producing beta cells [1, 2]. The molecular basis of this autoimmune beta cell destruction remains poorly understood. Autoantibodies specific for beta cell proteins arise early in life. The greater the number of antigen specificities recognised by these autoantibodies, the greater an individual’s risk of developing type 1 diabetes [3]. It is clear that CD4+ and CD8+ T cells are primarily responsible for beta cell destruction in type 1 diabetes. Many genetic loci have been described that are associated with increased risk of developing type 1 diabetes [4]. Of these, the strongest risk alleles are found in the HLA class II region, specifically HLA-DQ [5] and the insulin gene promoter [6]. The natural history of type 1 diabetes has been classified into three stages: stage 1 is characterised by the presence of autoantibodies specific for beta cell proteins; in stage 2, dysglycaemia develops in addition to autoantibody presence; at stage 3, an individual has symptomatic type 1 diabetes [7].
Autoimmunity, post-translational modifications and neoepitopes
Over the past decades, T cell responses against neoepitopes have become increasingly implicated in the pathogenesis of autoimmune diseases, including type 1 diabetes (reviewed in [1, 8,9,10]). Autoimmune T cell responses that are specific to neoepitopes formed in peripheral tissues may explain how and why T cell responses are not subject to the usual tolerance mechanisms; specifically, thymic deletion of self-reactive T cells and peripheral tolerance. The corollary of the ‘neoepitope hypothesis’, is that neoepitopes formed during cellular stress will challenge the immune system’s capacity to distinguish self from non-self. It may be that, when the cell is under physiological stress, these mechanisms are attenuated, leading to destructive autoimmunity in genetically susceptible individuals [11]. For example, endoplasmic reticulum (ER) stress leads to the modification of tyrosine phosphatase-related islet antigen 2 (IA-2), creating neoepitopes recognised by human CD4+ T cells [12].
Why is it important to define neoepitopes associated with type 1 diabetes?
Identification of the epitopes recognised by pathogenic human T cells in type 1 diabetes is important for both translational and basic research. For translational research, this information will support the development of assays that can monitor changes in the function and frequency of antigen-specific T cells from a blood sample. Neoepitopes that are known targets of pathogenic T cell responses will be prime candidates for incorporation into antigen-specific therapies to restore immune tolerance to beta cells. These goals go hand-in-hand. A suitably robust and sensitive assay to monitor changes in T cell numbers and function is essential for monitoring changes induced by experimental antigen-specific therapies [13].
The identification of epitopes recognised by pathogenic T cells in type 1 diabetes is also an important goal for basic research scientists. The elucidation of targets of the autoimmune T cell response against beta cells will address enduring questions about the immune pathogenesis of human type 1 diabetes [1]. Currently, it is not known why immune tolerance towards beta cells is lost in people who develop type 1 diabetes. Identifying the relevant T cell epitopes will help to reveal how pathogenic T cells avoid thymic deletion and peripheral tolerance mechanisms. These insights may explain many of the enigmatic features of the aetiology of type 1 diabetes, such as the long-known association between HLA-DQ2/DQ8 alleles and increased risk of developing type 1 diabetes [5, 14].
How to identify neoepitopes: approaches and challenges
Identifying neoepitopes recognised by T cells in people with, or at risk of type 1 diabetes continues to be difficult. The problem has three facets: to find (1) beta cell specific T cells, (2) the appropriate antigen and (3) the appropriate modification of that antigen.
Beta cell-specific T cells have been identified using three broad approaches; the first of these being functional analysis of human T cells. For example, T cells specific for relevant antigens/epitopes have been isolated from peripheral blood mononuclear cells (PBMCs) using the carboxyfluorescein succinimidyl ester (CFSE)-based proliferation assay [15], or HLA tetramers complexed with candidate neoepitopes [16]. In addition, human T cell-based approaches have recently been used to identify relevant T cells by their location within islets [17,18,19] (discussed in more detail below). Second, proteomic approaches, including peptide elution and mass spectrometry, have been used to identify potentially relevant modifications of beta cell proteins. The advantage of these approaches is that they identify modified proteins in a relatively unbiased manner, enabling unanticipated modifications to be identified (reviewed in [20]). For example, using 2D gel electrophoresis, glucose-regulated protein (GRP) 78 was found to be citrullinated in NOD mouse islets [21]. More recently, peptide elution from human beta cell lines has identified HLA-A2-restricted neoepitopes, formed by mRNA splice variants of beta cell antigens [22]. Third, some neoepitopes recognised by human T cells have first been identified in NOD mice. The best recent example of this is the discovery of hybrid insulin peptides (HIPs) [23], which were first identified as the targets of the pathogenic BDC T cells from NOD mice and then shown to be recognised by human islet-infiltrating CD4+ T cells.
Autoantibody responses against neoepitopes
While the analysis of immune responses to neoepitopes has focused on T cells, there is some evidence that autoantibodies specific for neoepitopes can be detected in people with type 1 diabetes. For example, autoantibodies specific for reactive oxygen species (ROS)-modified type II collagen were detected in HLA-DR4 positive people with type 1 diabetes [24]. A higher titre autoantibody response was detected against oxidised insulin compared with unmodified insulin in serum from people with type 1 diabetes [25]. Moreover, in a follow-up study, it was found that autoantibodies specific for oxidised insulin were detected in children before they developed type 1 diabetes (in stage 2 of development); more than 90% of children who had oxidised-insulin-specific autoantibodies went on to develop type 1 diabetes [26]. Together, these studies imply that oxidatively modified forms of insulin may arise and prime autoantibody responses in people who develop type 1 diabetes.
An overview of neoepitopes in type 1 diabetes
The neoepitopes currently implicated in type 1 diabetes development (summarised in Table 1) can result from the following processes: (1) modifications arising during antigen processing and presentation [27]; (2) conversion of glutamine to glutamate, or arginine to citrulline [12, 16, 18, 28]; (3) peptide fusion [18, 22, 23]; or (4) aberrant mRNA translation [22, 29]. It is already clear that multiple mechanisms lead to the development of neoepitopes recognised by type 1 diabetes-associated T cell responses.
Recent advances in type 1 diabetes-associated T cell neoepitopes
Neoepitopes implicated in the pathogenesis of human type 1 diabetes have been reviewed elsewhere [8,9,10, 30, 31]. Here we focus on some recent discoveries that reveal new mechanisms for the formation of neoepitopes recognised by T cells from individuals with type 1 diabetes.
HIPs
In 2016, Delong et al [23] reported that diabetes-associated CD4+ T cells from NOD mice recognised HIPs. These neoepitopes are formed by the fusion of two peptide fragments in beta cells. The HIPs reported by Delong and colleagues were all fusions of parts of proinsulin C-peptide with other beta cell-granule components, such as islet amyloid polypeptide (IAPP) 2 (reviewed in [10, 32]). The mechanism that leads to the formation of HIPs is unclear, but it is believed to result from transpeptidation (in a similar manner to the formation of ‘spliced’ CD8+ T cell epitopes) (reviewed in [32]). Although CD4+ T cells that responded to HIPs were first discovered in the NOD mouse, two laboratories have isolated human islet-infiltrating CD4+ T cells that respond to HIPs, including HLA-DQ8-restricted CD4+ T cell clones [23]. More recently, it has been reported that T cell responses to HIPs predict onset of diabetes in the NOD mouse model [33]. It will be of great interest to determine if this is also true in humans.
Neoepitopes recognised by islet-infiltrating T cells
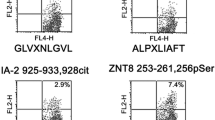
Building on our technique for isolating human islet-infiltrating T cells [17], Babon et al [18] reported that islet-infiltrating CD4+ T cells recognise a variety of neoepitopes. T cell lines recognised HIPs formed by the fusion of proinsulin C-peptide with peptides from insulin A-chain, IAPP1 and IAPP2. In addition, they found islet-infiltrating CD4+ T cells that responded to neoepitopes incorporating citrulline in place of arginine, specifically, GRP78292–305 with citrulline at position 297. This finding provides evidence that this neoepitope, which was first identified in the NOD mouse [21], may play a role in the pathogenesis of type 1 diabetes in humans. CD4+ T cell responses were also detected against IAPP65–84 with citrulline at positions 73 and 81. In almost all cases, the responses to a particular neoepitope were only found in a single individual (i.e. the neoepitope was only defined with the analysis of islet-infiltrating T cells from one person), suggesting that each individual may respond to a unique or restricted set of neoepitopes. Data on HLA restriction was not reported in this study, so it is unclear if these neoepitopes are presented by type 1 diabetes-associated HLA molecules [18]. Extensive T cell receptor (TCR) sequencing from human islet-infiltrating T cells has revealed a wide range of TCR genes used by these cells [34]. Pairing TCR sequencing with the analysis of neoepitope specificity will facilitate the dissection of neoepitope-specific T cell responses in human islets.
Alternative reading frames
Kracht et al [29] described neoepitopes derived from the insulin gene (INS) encoded by a non-canonical reading frame. CD4+ and CD8+ T cell responses were described against peptides that were formed by translation initiation 341 nucleotides downstream (3′) of the canonical start codon. Using this non-canonical start codon results in a different reading frame allowing translation to ‘read through’ the canonical stop codon. In this way the INS gene encodes a new polypeptide and, as a consequence, potential neoepitopes. Importantly, Kracht et al reported type 1 diabetes-associated CD4+ cells against the first nine amino acids (MLYQHLLPL) of the alternative reading frame INS gene product and HLA-A2-restricted responses against the same epitope. This study was the first to describe neoepitopes formed by translation from an alternative start codon. It will be of great interest to determine if non-canonical start codons result in the expression of neoepitopes from other beta cell-associated genes.
Elution and analysis of epitopes from HLA class I
Gonzalez-Duque et al [22] used transcriptomics and peptide elution to thoroughly characterise beta cell-derived epitopes presented by HLA class I. After identifying candidate epitopes, antigen-specific T cells were identified by HLA-A2 tetramer staining. From this work, in addition to many conventional epitopes, an HLA-A2-restricted hybrid epitope was identified, which was formed by the fusion of IAPP15–17 with IAPP5–10. Interestingly, several epitopes that resulted from mRNA splice variants of beta cell proteins were also identified. In the majority of cases, alternatively spliced mRNA levels were not increased after exposure to inflammatory cytokines (IFN-γ, TNF-α and IL-1β).
Opportunities and challenges for therapeutic intervention
From our growing understanding of the natural history of human type 1 diabetes, it is now clear that autoimmune T- and B cell responses arise early in life (stage 1 of type 1 diabetes development) [35], often many years before clinical disease (stage 3) manifests. The timing of the emergence of autoimmune T cell responses to neoepitopes is not yet known. The hypothesis that pathogenic T cell responses against neoepitopes arise very early in the course of type 1 diabetes, or even initiate the autoimmune responses against beta cells, is attractive. However, currently there is no experimental evidence to support this hypothesis. Recent evidence suggests that changes in the gene expression pattern of naive proinsulin- and GAD-responsive CD4+ T cells may precede the appearance of autoantibodies [35]. These observations suggest that responses to unmodified antigens arise very early in the course of disease. How T- and B cell responses to neo-epitopes evolve, and the capacity of these cells to respond to unmodified antigens, remains to be elucidated. A more detailed understanding of the dynamics of beta cell antigen-specific autoimmune responses may support the development of antigen-specific therapies.
With a growing list of neoepitopes, how can those best for T cell assays and antigen-specific therapies be identified? Ideally, the focus should be on the epitopes for which there is the strongest evidence for recognition by pathogenic T cells. At this stage, as discussed above, it is not known if any neoepitopes are the targets of pathogenic T cell responses in stage 1 or stage 2 of type 1 diabetes [7]. However, circumstantial evidence, such as being the targets of islet-infiltrating T cells, is also helpful; in particular those neoepitopes that are also restricted by HLA-DQ2/DQ8 should be on the ‘short list’. We suggest that there will not be a single ‘magic bullet’ but, instead, a panel of epitopes (both neoepitopes and conventional ones) will be required to measure and attenuate the full range of T cell responses against beta cells present in people who develop, or who are at risk of, type 1 diabetes.
Determining which neoepitopes are clinically relevant, i.e. the targets of pathogenic T cell responses, is difficult. Ideally, immunologists will be able to fulfil Koch’s postulates [36], by showing that T cells that recognise a particular neoepitope cause type 1 diabetes. Clearly, this is not possible in humans. One option is to develop a murine model of the human T cell response to beta cell antigens. While there have been some attempts [37, 38], to our knowledge there are no mouse models where a human TCR, specific for the human form of a beta cell antigen presented by HLA molecules, causes autoimmune diabetes. Hence, the pathogenicity of neoepitope-specific T cells remains to be directly determined.
The ultimate goal is to use neoepitopes in a form of antigen-specific therapy to curb the autoimmune T cell responses that drive beta cell destruction. Some allergic diseases have been treated with antigen-specific therapies [39]. Although type 1 diabetes has a different aetiology, in principle, progress in the field of allergy gives support to the notion that delivery of a disease-causing antigen/epitope in the appropriate format can be clinically beneficial. In type 1 diabetes, it is likely that giving antigen-specific therapy during stage 1 or stage 2 of the disease would be most effective because therapy delivered at these early stages may attenuate T cell responses against a presumably small number of (neo)epitopes, diffusing the autoimmune response before it can ‘spread’ to other antigens/epitopes. However, there are two barriers to this approach: (1) identifying the neoepitopes that are pivotal for autoimmunity during stages 1 and 2 of type 1 diabetes (it is more feasible to search for responses against neoepitopes in stage 3 of the disease); and (2) identifying individuals who are likely to benefit from such therapy before they show any symptoms of type 1 diabetes (stage 1 and 2 of the disease are asymptomatic). Alternatively, antigen-specific therapy could be given shortly after diagnosis of type 1 diabetes. In this scenario a panel of (neo)epitopes should be delivered to comprehensively suppress pathogenic T cell responses. Once the appropriate neoepitopes are identified, there are many emerging approaches that may be used to deliver these epitopes to induce or restore immunological tolerance (reviewed by [40, 41]).
Future directions in identifying and validating neoepitopes
Our challenge now is to develop high-throughput systems to identify neoepitopes and determine whether responses against neoepitopes drive autoimmune beta cell destruction in type 1 diabetes. New approaches for the identification of neoepitopes will need to accommodate the inconvenient truth that these molecules can be formed in a variety of ways [23, 29, 32], making neoepitope prediction almost impossible.
Although many challenges remain, neoepitopes have emerged as major new components in the type 1 diabetes puzzle over the past 15 years. Exciting new discoveries of novel mechanisms for neoepitope generation have greatly expanded our thinking and the possibilities for therapeutic intervention. With this progress, there is no doubt that the next 10–15 years will see a great increase in our knowledge of neoepitopes and the way in which they can be applied for improving the care of people with, or at risk of, type 1 diabetes.
Abbreviations
- GRP:
-
Glucose-regulated protein
- HIP:
-
Hybrid insulin peptides
- IAPP:
-
Islet amyloid polypeptide
- TCR:
-
T cell receptor
References
Mannering SI, Pathiraja V, Kay TW (2016) The case for an autoimmune aetiology of type 1 diabetes. Clin Exp Immunol 183(1):8–15. https://doi.org/10.1111/cei.12699
Pugliese A (2017) Autoreactive T cells in type 1 diabetes. J Clin Invest 127(8):2881–2891. https://doi.org/10.1172/JCI94549
Ziegler AG, Rewers M, Simell O et al (2013) Seroconversion to multiple islet autoantibodies and risk of progression to diabetes in children. JAMA 309(23):2473–2479. https://doi.org/10.1001/jama.2013.6285
Noble JA (2015) Immunogenetics of type 1 diabetes: a comprehensive review. J Autoimmun 64:101–112. https://doi.org/10.1016/j.jaut.2015.07.014
Todd JA, Bell JI, McDevitt HO (1987) HLA-DQβ gene contributes to susceptibility and resistance to insulin-dependent diabetes mellitus. Nature 329(6140):599–604. https://doi.org/10.1038/329599a0
Bennett ST, Lucassen AM, Gough SC et al (1995) Susceptibility to human type 1 diabetes at IDDM2 is determined by tandem repeat variation at the insulin gene minisatellite locus. Nat Genet 9(3):284–292. https://doi.org/10.1038/ng0395-284
Insel RA, Dunne JL, Atkinson MA et al (2015) Staging presymptomatic type 1 diabetes: a scientific statement of JDRF, the Endocrine Society, and the American Diabetes Association. Diabetes Care 38(10):1964–1974. https://doi.org/10.2337/dc15-1419
van Lummel M, Zaldumbide A, Roep BO (2013) Changing faces, unmasking the beta-cell: post-translational modification of antigens in type 1 diabetes. Curr Opin Endocrinol Diabetes Obes 20(4):299–306. https://doi.org/10.1097/MED.0b013e3283631417
James EA, Pietropaolo M, Mamula MJ (2018) Immune recognition of beta-cells: neoepitopes as key players in the loss of tolerance. Diabetes 67(6):1035–1042. https://doi.org/10.2337/dbi17-0030
Harbige J, Eichmann M, Peakman M (2017) New insights into non-conventional epitopes as T cell targets: The missing link for breaking immune tolerance in autoimmune disease? J Autoimmun 84:12–20. https://doi.org/10.1016/j.jaut.2017.08.001
Atkinson MA, Bluestone JA, Eisenbarth GS et al (2011) How does type 1 diabetes develop?: the notion of homicide or beta-cell suicide revisited. Diabetes 60(5):1370–1379. https://doi.org/10.2337/db10-1797
Marre ML, McGinty JW, Chow IT et al (2018) Modifying enzymes are elicited by ER stress, generating epitopes that are selectively recognized by CD4+ T cells in patients with type 1 diabetes. Diabetes 67(7):1356–1368. https://doi.org/10.2337/db17-1166
Herold KC, Brooks-Worrell B, Palmer J et al (2009) Validity and reproducibility of measurement of islet autoreactivity by T cell assays in subjects with early type 1 diabetes. Diabetes 58(11):2588–2595. https://doi.org/10.2337/db09-0249
Nepom GT, Kwok WW (1998) Molecular basis for HLA-DQ associations with IDDM. Diabetes 47(8):1177–1184. https://doi.org/10.2337/diab.47.8.1177
Mannering SI, Morris JS, Jensen KP et al (2003) A sensitive method for detecting proliferation of rare autoantigen-specific human T cells. J Immunol Methods 283(1-2):173–183. https://doi.org/10.1016/j.jim.2003.09.004
McGinty JW, Chow I-T, Greenbaum C, Odegard J, Kwok WW, James EA (2014) Recognition of posttranslationally modified GAD65 epitopes in subjects with type 1 diabetes. Diabetes 63(9):3033–3040. https://doi.org/10.2337/db13-1952
Pathiraja V, Kuehlich JP, Campbell PD et al (2015) Proinsulin-specific, HLA-DQ8, and HLA-DQ8-transdimer-restricted CD4+ T cells infiltrate islets in type 1 diabetes. Diabetes 64(1):172–182. https://doi.org/10.2337/db14-0858
Babon JA, DeNicola ME, Blodgett DM et al (2016) Analysis of self-antigen specificity of islet-infiltrating T cells from human donors with type 1 diabetes. Nat Med 22(12):1482–1487. https://doi.org/10.1038/nm.4203
Michels AW, Landry LG, McDaniel KA et al (2017) Islet-derived CD4 T cells targeting proinsulin in human autoimmune diabetes. Diabetes 66(3):722–734. https://doi.org/10.2337/db16-1025
Crevecoeur I, Rondas D, Mathieu C, Overbergh L (2015) The beta-cell in type 1 diabetes: what have we learned from proteomic studies? Proteomics Clin Appl 9(7-8):755–766. https://doi.org/10.1002/prca.201400135
Rondas D, Crevecoeur I, D’Hertog W et al (2015) Citrullinated glucose-regulated protein 78 is an autoantigen in type 1 diabetes. Diabetes 64(2):573–586. https://doi.org/10.2337/db14-0621
Gonzalez-Duque S, Azoury ME, Colli ML et al (2018) Conventional and neo-antigenic peptides presented by β cells are targeted by circulating naïve CD8+ T cells in type 1 diabetic and healthy donors. Cell Metab 28:1–15
Delong T, Wiles TA, Baker RL et al (2016) Pathogenic CD4 T cells in type 1 diabetes recognize epitopes formed by peptide fusion. Science 351(6274):711–714. https://doi.org/10.1126/science.aad2791
Strollo R, Rizzo P, Spoletini M et al (2013) HLA-dependent autoantibodies against post-translationally modified collagen type II in type 1 diabetes mellitus. Diabetologia 56(3):563–572. https://doi.org/10.1007/s00125-012-2780-1
Strollo R, Vinci C, Arshad MH et al (2015) Antibodies to post-translationally modified insulin in type 1 diabetes. Diabetologia 58(12):2851–2860. https://doi.org/10.1007/s00125-015-3746-x
Strollo R, Vinci C, Napoli N, Pozzilli P, Ludvigsson J, Nissim A (2017) Antibodies to post-translationally modified insulin as a novel biomarker for prediction of type 1 diabetes in children. Diabetologia 60(8):1467–1474. https://doi.org/10.1007/s00125-017-4296-1
Mannering SI, Harrison LC, Williamson NA et al (2005) The insulin A-chain epitope recognized by human T cells is posttranslationally modified. J Exp Med 202(9):1191–1197. https://doi.org/10.1084/jem.20051251
van Lummel M, Duinkerken G, van Veelen PA et al (2014) Posttranslational modification of HLA-DQ binding islet autoantigens in type 1 diabetes. Diabetes 63(1):237–247. https://doi.org/10.2337/db12-1214
Kracht MJ, van Lummel M, Nikolic T et al (2017) Autoimmunity against a defective ribosomal insulin gene product in type 1 diabetes. Nat Med 23(4):501–507. https://doi.org/10.1038/nm.4289
McGinty JW, Marre ML, Bajzik V, Piganelli JD, James EA (2015) T cell epitopes and post-translationally modified epitopes in type 1 diabetes. Curr Diab Rep 15(11):90. https://doi.org/10.1007/s11892-015-0657-7
Roep BO, Kracht MJ, van Lummel M, Zaldumbide A (2016) A roadmap of the generation of neoantigens as targets of the immune system in type 1 diabetes. Curr Opin Immunol 43:67–73. https://doi.org/10.1016/j.coi.2016.09.007
Mannering SI, So M, Elso CM, Kay TWH (2018) Shuffling peptides to create T cell epitopes: does the immune system play cards? Immunol Cell Biol 96(1):34–40. https://doi.org/10.1111/imcb.1015
Baker RL, Jamison BL, Wiles TA et al (2018) CD4 T cells reactive to hybrid insulin peptides are indicators of disease activity in the NOD mouse. Diabetes 67(9):1836–1846. https://doi.org/10.2337/db18-0200
Seay HR, Yusko E, Rothweiler SJ et al (2016) Tissue distribution and clonal diversity of the T and B cell repertoire in type 1 diabetes. JCI Insight 1:e88242
Heninger AK, Eugster A, Kuehn D et al (2017) A divergent population of autoantigen-responsive CD4+ T cells in infants prior to beta cell autoimmunity. Sci Transl Med 9(378):eaaf8848. https://doi.org/10.1126/scitranslmed.aaf8848
Koch R (1882) Die Aetiologie der Tuberculose. Berl Klin Wscht 19:221 [article in German]
Viehmann Milam AA, Maher SE, Gibson JA et al (2014) A humanized mouse model of autoimmune insulitis. Diabetes 63(5):1712–1724. https://doi.org/10.2337/db13-1141
Tan S, Li Y, Xia J et al (2017) Type 1 diabetes induction in humanized mice. Proc Natl Acad Sci U S A 114(41):10954–10959. https://doi.org/10.1073/pnas.1710415114
Curin M, Khaitov M, Karaulov A et al (2018) Next-generation of allergen-specific immunotherapies: molecular approaches. Curr Allergy Asthma Rep 18(7):39. https://doi.org/10.1007/s11882-018-0790-x
Serra P, Santamaria P (2015) Nanoparticle-based autoimmune disease therapy. Clin Immunol 160(1):3–13. https://doi.org/10.1016/j.clim.2015.02.003
Smith EL, Peakman M (2018) Peptide immunotherapy for type 1 diabetes-clinical advances. Front Immunol 9:392. https://doi.org/10.3389/fimmu.2018.00392
Funding
Work in the authors’ laboratory is supported by: JDRF [JDRF 5-CDA-2014-210-A-N] (SM); The National Health and Medical Research Council (NHMRC GNT123586) (SM); Diabetes Australia Research Trust Millennium Award (Y17M1-MANS) (SM); Diabetes Australia Research Program (Y18G-ELSC) (CE); and the Operational Infrastructure Support Program of the Victorian Government (SM, AD and CE). The authors have no financial conflicts to declare.
Author information
Authors and Affiliations
Contributions
All authors were responsible for drafting the article and revising it critically for important intellectual content. All authors approved the version to be published.
Corresponding author
Ethics declarations
The authors declare that there is no duality of interest associated with this manuscript.
Rights and permissions
About this article

Cite this article
Mannering, S.I., Di Carluccio, A.R. & Elso, C.M. Neoepitopes: a new take on beta cell autoimmunity in type 1 diabetes. Diabetologia 62, 351–356 (2019). https://doi.org/10.1007/s00125-018-4760-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-018-4760-6