
Abstract
Purpose
Stabilizing techniques for flail chest injuries are described through wide surgical approaches to the chest wall, especially in the most affected posterior and lateral regions. Severe morbidity due to these invasive approaches needs to be considered due to dissection of the scapular guiding muscles and the risk of injuries to neurovascular bundles. This study discusses possibilities for minimized approaches to the posterior and lateral regions.
Method
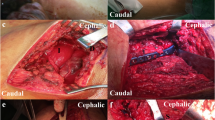
Ten fresh-frozen cadavers in lateral decubitus position were observed on both sides. Each surgical arm was kept mobile during the procedure. Approaches were performed following a standard protocol with muscle-sparing incisions starting with 5 cm in length and extending to 10 and 15 cm. The accessible surface comparing the extensions was measured. Visible ribs were counted. In a next step, MatrixRib® Plates were fixed to those ribs to prove the feasibility of rib stabilization through limited approaches.
Results
Combinations of the posterior and lateral minimized approaches allow surgical fixation of 6–9 and 7–11 ribs through 5 and 10 cm incisions, respectively. In the case of an extreme expansion of a rib fracture series, an access extension can be made to 15 cm to be able to adequately supply the entire hemithorax using two approaches.
Conclusion
Extensive invasive surgical approaches to the thoracic wall can be replaced by reduced invasive and muscle-sparing access combinations. A free-moving positioning of the arm and an accurate preoperative plan for minimizing approaches are essential. Minimally invasive plate techniques are very helpful adjuncts.







Similar content being viewed by others


Abbreviations
- Ap:
-
Anterior–posterior direction
- Cc:
-
Cranial–caudal direction
- Cm:
-
Centimeter
- Cm2 :
-
Square centimeter
- FC:
-
Flail chest
- L:
-
Left side
- Max:
-
Maximum
- Min:
-
Minimum
- MIPO:
-
Minimally invasive plate osteosynthesis
- Mm:
-
Millimeter
- π:
-
Pi = 3.14159265359
- R:
-
Right side
- SD:
-
Standard deviation
References
Leinicke JA, Elmore L, Freeman BD, Colditz GA. Operative management of rib fractures in the setting of flail chest: a systematic review and meta-analysis. Ann Surg. 2013;258(6):914–21.
Schuurmans J, Goslings JC, Schepers T. Operative management versus non-operative management of rib fractures in flail chest injuries: a systematic review. Eur J Trauma Emerg Surg 2017;43(2):163–8. https://doi.org/10.1007/s00068-016-0721-2.
NICE National Institute for Health and Clinical Excellence. Insertion of metal rib reinforcements to stabilise a flail chest wall. 2010 IPG361. http://egap.evidence.nhs.uk/IPG361.
Wiese MN, Kawel-Boehm N, Moreno de la Santa P, Al-Shahrabani F, Toffel M, Rosenthal R, Schäfer J, Tamm M, Bremerich J, Lardinois D. Functionall results after chest wall stabilization with a new screwless fixation device. Eur J Cardiothorac Surg 2015;47(5):868–75. https://doi.org/10.1093/ejcts/ezu318.
Pieracci FM, Majercik S, Ali-Osman F, Ang D, Doben A, Edwards JG, French B, Gasparri M, Marasco S, Minshall C, Sarani B, Tisol W, VanBoerum DH, White TW. Consensus statement: Surgical stabilization of rib fractures rib fracture colloquium clinical practice guidelines. Injury 2017;48(2):307–21. https://doi.org/10.1016/j.injury.2016.11.026.
Majercik S, Pieracci FM. Chest Wall Trauma. Thorac Surg Clin. 2017;27(2):113–21. https://doi.org/10.1016/j.thorsurg.2017.01.004.
Bottlang M, Long WB, Phelan D, Fielder D, Madey SM. Surgi- cal stabilization of fail chest injuries with MatrixRIB implants: a prospective observational study. Injury. 2013;44(2):232–8.
Clemens MW, Evans KK, Mardini S, Arnold PG. Introduction to chest wall reconstruction: anatomy and physiology of the chest and indications for chest wall reconstruction. Semin Plast Surg. 2011;25(1):5–15.
Gasparri MG, Tisol WB, Haasler GB. Rib stabilization: lessons learned. Eur J Trauma Emerg Surg. 2010;36:435–40.
Benninger E, Meier C. Minimally invasive lateral plate placement for metadiaphyseal fractures of the humerus and its implications for the distal deltoid insertion- it is not only about the radial nerve. A cadaveric study. Injury 2017;48(3):615–20. https://doi.org/10.1016/j.injury.2017.01.026.
Jiamton C, Apivatthakakul T. The safety and feasibility of minimally invasive plate osteosynthesis (MIPO) on the medial side of the femur: a cadaveric injection study. Injury 2015;46(11):2170–6. https://doi.org/10.1016/j.injury.2015.08.032.
Marasco S, Saxena P. Surgical rib fixation—technical aspects. Injury 2015;46(5):929–32. https://doi.org/10.1016/j.injury.2014.12.021.
Nickerson TP, Kim BD, Zielinski MD, Jenkins D, Schiller HJ. Use of a 90° drill and screwdriver for rib fracture stabilization. World J Surg 2015;39(3):789–793. https://doi.org/10.1007/s00268-014-2862-y.
Bemelman M, van Baal M, Yuan JZ, Leenen L. The role of minimally invasive plate osteosynthesis in rib fixation: a review. Korean J Thorac Cardiovasc Surg 2016;49(1):1–8. https://doi.org/10.5090/kjtcs.2016.49.1.1.
Schulz-Drost S, Oppel P, Grupp S, et al. Bony injuries of the thoracic cage in multiple trauma : Incidence, concomitant injuries, course and outcome. Unfallchirurg. 2016;119(12):1023–30 (in German).
Schulz-Drost S, Krinner S, Langenbach A, Oppel P, Lefering R, Taylor D, Hennig FF, Mauerer A, TraumaRegister DGU. Concomitant sternal fracture in flail chest: an analysis of 21,741 polytrauma patients from the TraumaRegister DGU®. Thorac Cardiovasc Surg 2017. https://doi.org/10.1055/s-0037-1598194.
Schulz-Drost S, Grupp S, Pachowsky M, Oppel P, Krinner S, Mauerer A, Hennig FF, Langenbach A. Stabilization of flail chest injuries: minimized approach techniques to treat the core of instability. Eur J Trauma Emerg Surg. 2017;43(2):169–78. https://doi.org/10.1007/s00068-016-0664-7.
Mohty KM, Cravens MG, Adamas-Rappaport WJ, Amini-Shervin B, Irving SC, Stea N, Adhikari S, Amini R. Cadaver-based necrotizing fasciitis model for medical training. Cureus 2017;9(4):e1168. https://doi.org/10.7759/cureus.1168.
Acknowledgements
Prior presentation of this study. Parts of this study were previously presented as a poster presentation by the first author AL at the German Congress for Orthopedics and Trauma Surgery in October 2015 (DKOU 2015, Berlin, Germany) and at the 16th European Congress for Trauma and Emergency Surgery in May 2015 (ECTES, Amsterdam, The Netherlands) in an oral talk by the senior author SSD. The surgical technique had been recently shown by the senior author during a webcast of the AO Foundation with a large number of international participants (AOTrauma Webcast: “Rib Fracture Osteosynthesis—Approaches and Management in the Different Sectors of the Chest Wall”, June 7 / 8, 2017, AMTS Muttenz, Switzerland; main presenter: Stefan Schulz-Drost).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The senior author has a consultant agreement with DePuySynthes and he is an advisory member of the AO TK Thoracic Surgery Expert Group (THEG). The other authors are not involved in any conflict of interest.
Funding
No funds were received in connection to this study.
Rights and permissions
About this article

Cite this article
Langenbach, A., Oppel, P., Grupp, S. et al. Reduced invasive and muscle-sparing operative approaches to the posterolateral chest wall provide an excellent accessibility for the operative stabilization!. Eur J Trauma Emerg Surg 44, 471–481 (2018). https://doi.org/10.1007/s00068-017-0877-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-017-0877-4