
Abstract
Purpose
Reconstruction of the facial midplane is relevant in anthropometry, orthodontics, maxillofacial surgery, and the accurate measurement of symmetry deviation is relevant in many fields of medicine especially when planning surgical treatment. In the literature, three different means of midplane generation have been published; however, there is currently no consensus regarding the approach to use. Morphometric methods are used to determine the true midsagittal plane (MSP), but its use in clinical practice is difficult. A regression plane based on N‑ANS-PNS landmarks reportedly approximates the morphometric MSP. As these points are vulnerable, we investigated which combination of landmarks can be substituted in symmetric and asymmetric faces.
Patients and methods
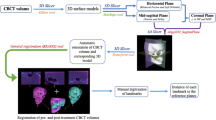
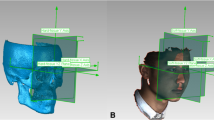
Thirty symmetric and 30 asymmetric faces were analyzed on cone-beam computed tomography scans. A total of 50 regression planes were generated based on three unpaired landmarks and 35 regression planes were generated based the midpoints of paired landmarks. The Na-ANS-PNS plane was used as reference plane, and the mean angle between it and each generated MSP was calculated. The differences from the reference plane were compared by t‑test between the groups.
Results
In the symmetric group, 86% of angles deviated by <5° using unpaired points, whereby 74% of angles deviated by <5° for paired points. Between the two groups 50% of planes from midline points, and 77% of planes from paired points were significantly different. All planes deviated more in the asymmetric group.
Conclusions
The N‑ANS-PNS reference plane can be substituted with the following combinations: ANS-G-Ba, ANS-G-S, ANS-S-De, PNS-G-Ba, PNS-S-Ba, PNS-ANS-G, and PNS-N-Ba.
Zusammenfassung
Ziel
Die Rekonstruktion der Gesichtsmittelebene ist von Bedeutung in der Anthropometrie, der Kieferorthopädie sowie der Mund‑, Kiefer- und Gesichtschirurgie. In vielen Bereichen der Medizin ist die genaue Bestimmung einer Symmetrieabweichung relevant, insbesondere bei der Planung chirurgischer Interventionen. In der Literatur wurden drei Verfahren zur Bestimmung der Midsagittalebene veröffentlicht, es gibt jedoch keinen Konsens über die Vorgehensweise. Zur Bestimmung der tatsächlichen mittsagittalen Ebene („true midsagittal plane“, MSP) werden morphometrische Methoden eingesetzt, die sich jedoch in der Klinik schwer umsetzen lassen. Berichtet wird, dass sich eine auf N‑ANS-PNS basierende Regressionsebene der morphometrischen MSP nähert. Wegen der Vulnerabilität dieser Punkte wurde untersucht, welche Kombination von Referenzpunkten sich bei symmetrischen bzw. asymmetrischen Gesichtern ersatzweise eignet.
Patienten und Methoden
Es wurden insgesamt 60DVTs ausgewertet: 30 von symmetrischen und 30 von asymmetrische Gesichtern. Basierend auf drei unpaarigen Referenzpunkten wurden insgesamt 50 Regressionsebenen generiert, 35 Regressionsebenen basierten auf den gemittelten paarigen Referenzpunkten. Als Bezugsebene wurde die Na-ANS-PNS-Ebene verwendet und der mittlere Winkel zwischen dieser und jedem erzeugten MSP wurde berechnet. Die Unterschiede zur Bezugsebene zwischen den Gruppen wurden mittels t‑Test evaluiert.
Ergebnisse
In der symmetrischen Gruppe wichen 86 % der Winkel um <5° bei unpaarigen Punkten ab, 74 % der Winkel wichen bei paarigen Punkten um <5° ab. Zwischen beiden Gruppen waren 50 % der Ebenen von Mittellinienpunkten und 77 % der Ebenen von gepaarten Punkten signifikant unterschiedlich. Alle Ebenen wichen in der asymmetrischen stärker als in der symmetrischen Gruppe ab.
Schlussfolgerungen
Die N‑ANS-PNS-Referenzebene kann durch folgende Kombinationen ersetzt werden: ANS-G-Ba, ANS-G-S, ANS-S-De, PNS-G-Ba, PNS-S-Ba, PNS-ANS-G und PNS-N-Ba.




Similar content being viewed by others

References
Aoshima O (1990) Investigation of the facial symmetry of cases with cross bites needing surgical orthodontic treatment using postero-anterior roentgenographic cephalometrics. Nihon Kyosei Shika Gakkai Zasshi 49:256–262
Bajaj K, Rathee P, Jain P, Panwar VR (2011) Comparison of the reliability of anatomic landmarks based on PA cephalometric radiographs and 3D CT scans in patients with facial asymmetry. Int J Clin Pediatr Dent 4:213–223
Bajwa RA, Mehmood F, Jalil S (2012) Frequency and etiology of different types of nasal bones fracture reporting at a tertiary care centre, Lahore, Pakistan. J Med Sci 6:703–709
Cho J‑H, Moon J‑Y (2010) Comparison of midsagittal reference plane in PA cephalogram and 3D CT. Korean J Orthod 40:6–15
Choi KY (2015) Analysis of facial asymmetry. Arch Craniofac Surg 16:1–10
Damstra J, Fourie Z, De Wit M, Ren Y (2012) A three-dimensional comparison of a morphometric and conventional cephalometric midsagittal planes for craniofacial asymmetry. Clin Oral Investig 16:285–294
Escada P, Penha RS (1999) Fracture of the anterior nasal spine. Rhinology 37:40–42
Haraguchi S, Takada K, Yasuda Y (2002) Facial asymmetry in subjects with skeletal class III deformity. Angle Orthod 72:28–35
Harsh M, Gowdra S, Maurya RK (2014) Assessment of facial asymmetry in various malocclusion: a comparative analysis. J Indian Orthod Soc 48:534–545
Jacobson A, Jacobson RL (2006) Radiographic cephalometry: from basics to 3‑D imaging. Quintessence, New Malden
Lisboa Cde O, Masterson D, da Motta AF, Motta AT (2015) Reliability and reproducibility of three-dimensional cephalometric landmarks using CBCT: a systematic review. J Appl Oral Sci 23:112–119
Major PW, Johnson DE, Hesse KL, Glover KE (1994) Landmark identification error in posterior anterior cephalometrics. Angle Orthod 64:447–454
Raggio BS, Graham HD (2017) Fracture of the anterior nasal spine: a systematic review. J Oral Maxillofac Surg Med Pathol. https://doi.org/10.1016/j.ajoms.2017.09.008
Schlicher W, Nielsen I, Huang JC, Maki K, Hatcher DC, Miller AJ (2012) Consistency and precision of landmark identification in three-dimensional cone beam computed tomography scans. Eur J Orthod 34:263–275
Sicurezza E, Greco M, Giordano D, Maiorana F, Leonardi R (2012) Accuracy of landmark identification on postero-anterior cephalograms. Prog Orthod 13:132–140
Shin SM, Kim YM, Kim NR, Choi YS, Park SB, Kim YI (2016) Statistical shape analysis-based determination of optimal midsagittal reference plane for evaluation of facial asymmetry. Am J Orthod Dentofacial Orthop 150:252–260
Swennen GRJ (2010) Three-dimensional cephalometry: a color atlas and manual. Springer, Berlin
Thiesen G (2016) Determining the midsagittal reference plane for evaluating facial asymmetries. Am J Orthod Dentofacial Orthop 150:908–909
Wong TY, Liu JK, Fang JJ, Wu TC, Tu YH (2014) Use of the matching optimal symmetry plane method in planning surgical correction of facial asymmetry—a preliminary report of 20 patients. J Oral Maxillofac Surg 72(1180):e1–e13
Acknowledgements
We would like to thank Editage (www.editage.com) for English language editing. This study was supported by the ÚNKP-17-3 New National Excellence Program of the Ministry of Human Capacities of Hungary.
Funding
This study was supported by the ÚNKP-17-3 New National Excellence Program of the Ministry of Human Capacities of Hungary.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
A. Dobai, Z. Markella, T. Vízkelety, C. Fouquet, A. Rosta and J. Barabás declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Dobai, A., Markella, Z., Vízkelety, T. et al. Landmark-based midsagittal plane analysis in patients with facial symmetry and asymmetry based on CBCT analysis tomography. J Orofac Orthop 79, 371–379 (2018). https://doi.org/10.1007/s00056-018-0151-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00056-018-0151-3