
Summary
Objectives
To investigate the hospital length of stay (LOS) and total direct costs of management of patients with intracranial aneurysm in Italy. To test whether treatment choices impact LOS and total direct costs.
Design
Data were collected in a prospective, incidence-based, observational multicentre study. Patients were enrolled in a consecutive manner in 27 hospitals stratified according to macro-areas (North, Centre and South) and volume of activity (number of aneurysm patients treated annually). The costs were evaluated through a bottom-up, microcosting approach. The associations between demographic characteristics, clinical variables, modality of treatment and LOS/total costs were examined in two multiple regression models.
Results
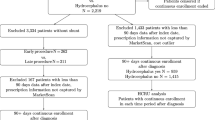
A total of 473 patients with single aneurysm were enrolled from October 1st 2005 to November 30th 2006 across the country. The average length of stay was 19.8 days while the total direct costs per patient were €21,810. The overheads represented the most important cost category (€15,867), followed by supplies used during treatment procedure (€3026), personnel (€1042) and diagnostic imaging (€591). Fifty four % of patients were treated with endovascular (coiling) approach while the rest was submitted to surgical intervention (clipping). After adjusting for covariates, three significant predictors of hospital LOS were identified: Hunt & Hess (H&H) level, geographical area and choice of treatment, while the type of admitting organizational unit represented one additional predictor of total costs. One additional point on H&H scale resulted in increasing LOS by 14% (p<0.001) and total costs by 16% (p<0.001), holding other variables constant. The choice of treatment also predicts the outcome: endovascular approach decreases LOS by 39% (p=0.001) without significant reduction of total costs (p=0.4).
Conclusions
The intracranial aneurysm treatment poses significant economic burden on hospitals. The current analysis indicates that choice of endovascular therapy is associated with decreased hospital length of stay.
Similar content being viewed by others


Bibliografia
Michaud CM, Christopher M, Bloom B. Burden of disease-implications for future research. JAMA 2001; 285: 535–9
OMS. The Top Ten Causes of Death. The Ten Leading Causes of Death by Broad Income Group 2002. Fact Sheet N. 310, February 2007
Teunissen LL, Rinkel GJE, Algra A, Van Gijn J. Risk factors for subarachnoid hemorrhage: a systematic review. Stroke 1996; 27: 544–9
Woo D, Haverbusch M, Sekar P, et al. Effect of untreated hypertension on hemorrhagic stroke. Stroke 2004; 35: 1703–8
Rinkel GJE, Djibuti M, Algra A, Van Gijn J. Prevalence and risk of rupture of intracranial aneurysms: a systematic review. Stroke 1998; 29: 251–6
Higashida RT, Lahue BJ, Torbey MT, et al. Treatment of unrupted intracranial aneurysms: a nationwide assessment of effectiveness. AJNR Am J Neuroradiol 2007; 28: 146–51
Linn FH, Rinkel GJ, Algra A, Van Gijn J. Incidence of subarachnoid haemorrhage: role of region; year and rate of computed tomography: a meta-analysis. Stroke 1996; 27: 625–9
Wiebers DO, Torner JC, Meissner I. Impact of unruptured intracranial aneurysms on public health in the United States. Stroke 1992; 23: 1416–9
Molyneux A, Kerr R, ISAT Collaborative Group. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. J Stroke Cerebrovasc Dis 2002; 11: 304–14
ISAT Collaborative Group. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet 2002; 360: 1267–74
Molyneux AJ, Kerr RSC, Yu L-M, et al. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005; 366: 809–17
Campi A, Ramzi N, Molyneux AJ, et al. Retreatment of ruptured cerebral aneurysms in patients randomized by coiling or clipping in the International Subarachnoid Aneurysm Trial (ISAT). Stroke 2007; 38: 1538–44
NICE. Coil Embolisation of Ruptured Intracranial Aneurysms. Interventional Procedure Guidance 106. London: NHS, February 2005
NICE. Coil Embolisation of Ruptured Intracranial Aneurysms. Understanding NICE Guidance — Information for People Considering the Procedure, and for the Public. London: NHS, January 2005
Choudhari KA, Ramachandran MS, McCarronb MO, Kaliaperumal C. Aneurysms unsuitable for endovascular intervention: surgical outcome and management challenges over a 5-year period following International Subarachnoid Haemorrhage Trial (ISAT). Clin Neurol Neurosurg 2007; 109: 868–75
Kieran M. ISAT and ISUIA: the impact on informed consent. Tech Vasc Interv Radiol. 2005; 8: 106–7
Gnanalingham KK, Apostolopoulos V, Barazi S, O’Neil K. The impact of the international subarachnoid aneurysm trial (ISAT) on the management of aneurysmal subarachnoid haemorrhage in a neurosurgical unit in the UK. Clin Neurol Neurosurg 2006; 108: 117–23
Johnston SC. Effect of endovascular services and hospital volume on cerebral aneurysm treatment outcome. Stroke 2000; 31: 111–7
Koivisto T, Vanninen R, Hurskainen H, et al. Outcomes of early endovascular versus surgical treatment of ruptured cerebral aneurysm: a prospective randomized study. Stroke 2000; 31: 2369–77
Niskanen M, Koivisto T, Ronkainen A, et al. Resource use after subarachnoid hemorrhage: comparison between endovascular and surgical treatment. Neurosurgery 2004; 54: 1081–8
Roos YB, Dijkgraaf MG, Albrecht KW, et al. Direct costs of modern treatment of aneurysmal subarachnoid haemorrhage in the first year after diagnosis. Stroke 2002; 33: 1595–9
Javadpour M, Jain H, Wallace C, et al. Analysis of cost related to clinical and angiographic outcomes of aneurysm patients enrolled in the International Subarachnoid Aneurysm Trial in a North American setting. Neurosurgery 2005; 56: 886–94
Tarricone R. Valutazioni economiche e management in sanità. Milano: McGraw-Hill, 2004
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Torbica, A., Tarricone, R., Calciolari, S. et al. Analisi dei costi del trattamento dell’aneurisma intracranico in Italia. Pharmacoeconomics-Ital-Res-Articles 11, 25–37 (2009). https://doi.org/10.1007/BF03320655
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03320655