
Abstract
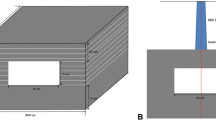
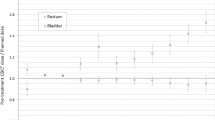
In IMRT treatment, margin for planning target volume is determined by organ motion and set-up error. The margin width that achieves the desired dose escalation, while minimizing normal tissue exposure is dependent upon patient immobilization and/or organ localization techniques. In this study, we compare the impact of margin width on the dosimetry of tumour and normal tissues using an endorectal balloon filled with 100 cc of air. Plans were generated for ten patients using margin widths of 0, 3, 5, 8 and 10 mm. The prescription dose to prostate and seminal vesicles was 70 Gy in 35 fractions with 15% of bladder allowed to receive above 65 Gy, 15% of rectum above 68 Gy and 10% of femurs above 45 Gy. Margins above 5 mm produced significantly lower mean doses for both prostate and seminal vesicles without affecting TCP. For normal tissues, mean doses, percent volumes above prescription constraints and NTCP increased as a function of margin width, especially when this was 5 mm or above. We conclude that planning with tighter margins of ≤5 mm improves IMRT dosimetry for prostate and normal tissues and is only possible when target localization and/or immobilization devices are routinely used.
Similar content being viewed by others

References
Ghilezan, M., Yan, D., Liang, J., Jaffray, D., and Wong, M. A.,Online image-guided intensity-modulated radiotherapy for prostate cancer: How much improvement can we expect? A theoretical assessment of clinical benefits and potential dose escalation by improving precision and accuracy of radiation delivery, Int. J. Radiat. Oncol. Biol. Phys., 60(5):1602–1610, 2004, and references therein.
Teh, B. S., Woo, S. Y., Mai, W. Y., Mc Gary, J. E., Carpenter, L. S., Lu, H. H., Chiu, J. K., Vlachaki, M. T., Grant, W. H. III and Butler, E. B.,Clinical experience with intensity-modulated radiation therapy (IMRT) for prostate cancer with the use of rectal balloon for prostate immobilization, Med. Dosim., 27(2):105–113, 2002.
Teh, B. S., Mai, W. Y., Uhl, B. M., Augspurger, M. E., Grant, W. H. III, Lu, H. H., Woo, S. Y., Carpenter, L. S., Chiu, J. K. and Butler, E. B.,Intensity-Modulated Radiation Therapy (IMRT) for Prostate Cancer with the Use of a Rectal Balloon for Prostate Immobilization: Acute Toxicity and Dose-Volume Analysis, Int. J. Radiat. Oncol. Biol. Phys., 49(3):705–712, 2001.
Ahmad, S., Vlachaki, M. T., Teslow, T. N., Amosson, C. M., McGary, J., The, B. S., Woo, S. Y., Butler, E. B., and Grant, W. H. III,Impact of setup uncertainty in the dosimetry of prostate and surrounding tissues in prostate cancer patients treated with Peacock/IMRT, Med. Dosim., 30(1):1–7, 2005.
McGary, J. E. and Grant, W. H. III,A clinical evaluation of setup errors for a prostate immobilization system, J. Appl. Clin. Med. Phys., 1(4):138–147, 2000.
McGary, J. E., Teh, B. S., Butler, E. B. and Grant, W. H. III,Prostate immobilization using a rectal balloon, J. Appl. Clin. Med. Phys., 3(1):6–11, 2002.
Carol, M. P.,Beam Modulation Conformal Radiotherapy.In: Purdy, J. A., Emami, B., editors,3D Radiation Treatment Planning and Conformal Therapy, Advanced Medical Publishing, Madison, 435–445, 1993.
Grant, W. H. III,Experience with Intensity Modulated Beam Delivery.In: Mackie, T. R.; Palta, J. R., editors,Teletherapy: Present and Future, Advanced Medical Publishing; Madison, 793–804, 1996.
Sternick, E. S., Carol, M. P. and Grant, W. H. III,Intensity Modulated Radiotherapy.In:Khan, F. M., Potish, R. A., editors,Treatment Planning in Radiation Oncology, Williams and Wilkins, Baltimore, 187–213, 1998.
Niemierko, A.,Reporting and analyzing dose distribution: A concept of equivalent uniform dose, Med. Phys., 24:103–109, 1997.
Nahum, A. E. and Tait, D. M.,Maximizing tumour control by customized dose prescription for pelvic tumours in advanced radiation therapy: Tumour response monitoring and treatment planning, Breit, A., editor, Springer, Berlin, 425–431, 1992.
Lyman, J. T.,Complication probability as assessed from dose volume histograms, Radiat. Res. Suppl., 8:S13–19, 1985.
Kutcher, G. J. and Burman, C.,Calculation of complication probability factors for non uniform normal tissue irradiation: the effective volume method, Int. J. Radiat. Oncol. Biol. Phys., 16(6):1623–1630, 1989.
Burman, C., Kutcher, G. J., Emami, B. and Goitein, M.,Fitting of normal tissue tolerance data to an analytic function, Int. J. Radiat. Oncol. Biol. Phys., 21(1):123–135, 1991.
Emami, B., Lyman, J., Brown, A., Coia, L., Goitein, M., Munzenrider, J. E., Shank, B., Solin, L. J. and Wesson, M.,Tolerance of normal tissue to therapeutic irradiation, Int. J. Radiat. Oncol. Biol. Phys., 21(1):109–122, 1991.
Wang, J. Z., Li, X. A., Yu, C. X. and Dibiase, S. J.,The low α/β ratio for prostate cancer: what does the clinical outcome of HDR brachytherapy tell us?, Int. J. Radiat. Oncol. Biol. Phys., 57(4):1101–1108, 2003.
Vlachaki, M. T., Teslow, T. N., Amosson, C. M., Grant, W. H. and Butler, E. B.,Impact of endorectal balloon reposition in the dosimetry of prostate and surrounding normal tissues in patients with prostate cancer treated with the peacock/IMRT technique, Radiology, (S)217; 142, 2000.
Uhl, B. M., Teh, B. S., Wheeler, T., Scardino, P. T., Woo, S. Y. and Butler, E. B.,Intensity modulated radiation therapy IMRT for localized prostate cancer: a comparison of peacock conformal treatment volumes and pathologic radical prostatectomy specimens, Int. J. Radiat. Oncol. Biol. Phys., 42(1-suppl):292, 1998.
Teh, B. S., Bastasch, M. D., Wheeler, T. M., Mai, W. Y., Frolov, A., Uhl, B. M., Lu, H. H., Carpenter, L. S., Chiu, J. K., Mcgary, J., Woo, S. Y., Grant, W. H. and Butler, E. B.,IMRT for prostate cancer defining target volume based on correlated pathologic volume of disease, Int. J. Radiat. Oncol. Biol. Phys., 56:184–191, 2003.
Cox, J. D., Stetz, J. and Pajak, T. F.,Toxicity Criteria of the Radiation Therapy Oncology Group (RTOG) and then European Organization for Research and Treatment of Cancer (EORTC), Int. J. Radiat. Oncol. Biol. Phys., 31:1341–1346, 1995.
Hall, E. J.,Henry S. Kaplan Distinguished Scientist Award 2003, The crooked shall be made straight; dose-response relationships for carcinogenesis, Int. J. Radiat. Oncol. Biol., Phys., 80(5):327–337, 2004.
Brenner, D. J., Curtis, R. E., Hall, E. J. and Ron, E.,Second malignancies in prostate carcinoma patients after radiotherapy compared with surgery, Cancer, 88(2):398–406, 2000.
Hall, E. J. and Wuu, C. S.,Radiation-induced second cancers: the impact of 3D-CRT and IMRT, Int. J. Radiat. Oncol. Biol. Phys., 56(1):327–337, 2004.
Nutting, C. M., Corbishley, C. M., Sanchez-nieto, B., Cosgrove, V. P., Webb, S. and Dearnaley, D. P.,Potential improvements in the therapeutic ratio of prostate cancer irradiation: dose escalation of pathologically identified tumour nodules using intensity modulated radiotherapy, Brit. J. Radiol., 75:151–161, 2002.
Guerrero Urbano, M. T. and Nutting, C. M.,Clinical use of intensity-modulated radiotherapy: part II (Review Article), Brit. J. Radiol., 77:177–182, 2004.
Burman, C., Chui, C. S., Kutcher, G., Leibel, S., Zelefsky, M., LoSasso, T., Spirou, S., Wu, Q., Yang, J., Mohan, R., Fuks, Z. and Ling, C. C.,Planning, delivery, and quality assurance of intensity modulated radiotherapy using dynamic multileaf collimator: a strategy for large scale implementation for the treatment of carcinoma of the prostate, Int. J. Radiat. Oncol. Biol. Phys., 39:863–873, 1997.
Muren, L. P., Ekerold, R., Kvinnsland, Y., Karlsdottir, A. and Dahl, O.,On the use of margins for geometrical uncertainties around the rectum in radiotherapy planning, Radiother. Oncol., 70:11–19, 2004.
McKenzie, A., Van, H. M. and Mijnheer, B.,margins for geometric uncertainty around organs at risk in radiotherapy, Radiother. Oncol., 62:299–307, 2002.
ICRU Report 62,Prescribing, Recording, and Reporting Photon Beam Therapy, (Supplement to ICRU Report 50), Bethesda, MD, 1999.
Stroom, J. C. and Heijmen, B. J. M.,Geometrical uncertainties, radiotherapy planning margins, and the ICRU-62 report, Radiother. Oncol., 64:75–83, 2002.
Van, H. M., Remeijer, P., Rasch, C. and Lebesque, J. V.,The probability of correct target dosage: dose population histograms for deriving treatment margins in radiotherapy, Int. J. Radiat. Oncol. Biol. Phys., 47(4):1121–1135, 2000.
Manning, M. A., Wu, Q., Cardinale, R. M., Mohan, R., Lauve, A. D., Kavanagh, B. D., Morris, M. M. and Schmid-Ulrich, R. K.,The effect of setup uncertainty on normal tissue sparing with IMRT for head and neck cancer, Int. J. Radiat. Oncol. Biol. Phys., 51(5):1400–1409, 2001.
Wong, J. R., Grimm, L., Uematsu, M., Oren, R., Cheng, C. W. Merrick, S. and Schiff, P.,Image-guided radiotherapy for prostate cancer by CT-linear accelerator combination: prostate movements and dosimetric considerations, Int. J. Radiat. Oncol. Biol. Phys., 61(2):561–569, 2005.
Jaffray, D. A., Siewerdsen, J. H., Wong, J. W. and Matinez, A. A.,Flat-Panel cone beam computed tomography for image guided radiation therapy, Int. J. Radiat. Oncol. Biol. Phys., 53(5):1337–1349, 2002.
Beavis, A. W.,Is tomotherapy the future of IMRT?, Brit. J. Radiol., 77(916):285–295, 2004.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ahmad, S., Vlachaki, M.T. Impact of margin on tumour and normal tissue dosimetry in prostate cancer patients treated with IMRT using an endorectal balloon for prostate immobilization. Australas. Phys. Eng. Sci. Med. 28, 209–215 (2005). https://doi.org/10.1007/BF03178720
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03178720