
Abstract
Purpose
Inadvertent epidural needle punctures represent the leading cause of severe postdural puncture headache (PDPH) in parturients. Use of small gauge (G) epidural needles for continuous analgesia has received little attention despite possible important reductions in PDPH. We report the first study to examine the feasibility of using small G Tuohy needles and 23 G catheters for labour analgesia.
Methods
Healthy parturients ≤ 6 cm dilated were recruited. Epidural analgesia was established using a 19 G Tuohy epidural needle, a 23 G single port 40 cm catheter and bupivacaine 0.08% with fentanyl 2 µg·mL-1 (15-20 mL). Breakthrough pain was treated by protocol. There was no formal in-training period for anesthesiologists. The primary outcome was the combined failure rate for initiation (failed needle/catheter placement or failed block ≤ 30 min of drug administration). Secondary outcomes included late block failure (> 30 min), recognized dural puncture, PDPH, patient assessment of analgesia within 24 hr of delivery, complications and anesthesiologist satisfaction.
Results
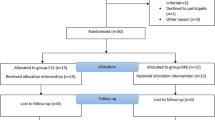
Twenty-seven parturients were recruited. Successful blocks were initiated and maintained in 24/27 who rated overall analgesia from good to excellent (19/24 very good to excellent). Three block failures occurred at the initiation phase only (two unilateral, one absent). There was no evidence of catheter kinking after placement. One patient developed PDPH after unrecognized dural puncture which was self-treated with acetaminophen for four days, followed by complete symptom resolution.
Conclusion
It is feasible to provide high quality labour analgesia using small G epidural needles and catheters. The effect of small G epidural needles on PDPH warrants future study.
Résumé
Objectif
La ponction péridurale involontaire représente la principale cause de céphalée postponction durale (CPPD) chez les parturientes. Ľusage ďaiguilles de petit calibre (G) pour ľanalgésie continue a reçu peu ďattention malgré la possibilité de réductions importantes de CPPD. Nous présentons la première étude qui vérifie la faisabilité de ľutilisation ďaiguilles Tuohy de petit G et de cathéters de 23 G pour ľanalgésie du travail obstétrical.
Méthode
Des parturientes saines chez qui la dilatation était ≤ 6 cm ont été recrutées. Ľanalgésie péridurale a été installée avec une aiguille Tuohy de 19 G, un cathéter de 40 cm à une seule ouverture de 23 G et de la bupivacaïne à 0,08 % et 2 µg·mL-1 de fentanyl (15-20 mL). La douleur persistante a été traitée selon le protocole. Il n’y a pas eu de formation formelle pour les anesthésiologistes. Le principal critère étudié était le taux ďéchec combiné pour ľinstallation (échec de la mise en place de ľaiguille/du cathéter ou échec du bloc ≤ 30 min après ľadministration du médicament). Les paramètres secondaires étaient ľéchec tardif du bloc (> 30 min), la ponction durale reconnue, les CPPD, ľévaluation de ľanalgésie par la patiente moins de 24 h après ľaccouchement, les complications et la satisfaction de ľanesthésiologiste.
Résultats
Vingt-sept parturientes ont été recrutées. Des blocs réussis ont été installés et maintenus chez 24/27 femmes qui ont évalué ľanalgésie de bonne à excellente (19/24 de très bonne à excellente). Trois échecs de bloc sont survenus à la phase initiale (deux unilatéraux et un absent). Aucune évidence de pliure n’a été relevée après la mise en place du cathéter. Une patiente a souffert de CPPD après une ponction durale involontaire qui a été traitée avec de ľacétaminophène pendant quatre jours et suivie ďune résolution complète des symptômes.
Conclusion
On peut fournir une analgésie de qualité pendant le travail en utilisant des aiguilles et des cathéters périduraux de petit G. Ľeffet des aiguilles de petit G sur les CPPD devra être précisé dans une future étude.
Similar content being viewed by others


References
Angle PJ, Kronberg J, Thompson D, et al. Dural tissue trauma and cerebrospinal fluid leak after epidural needle puncture: effect of needle design, angle and bevel orientation. Anesthesiology 2003; 99: 1376–82.
Aida S, Taga K, Yamakura T, Endoh H, Shimoji K. Headache after attempted epidural block: the role of intrathecal air. Anesthesiology 1998; 88: 76–81.
Stride PC, Cooper GM. Dural taps revisited. A 20-year survey from Birmingham Maternity Hospital. Anaesthesia 1993; 48: 247–55.
Angle P, Tang SL, Thompson D, Szalai JP. Expectant management of postdural puncture headache increases hospital length of stay and emergency room visits. Can J Anesth 2005; 52: 397–402.
Angle P, Thompson D, Halpern S, Wilson DB. Second stage pushing correlates with headache after unintentional dural puncture in parturients. Can J Anesth 1999; 46: 861–6.
Paech M, Banks S, Gurrin L. An audit of accidental dural puncture during epidural insertion of a Tuohy needle in obstetric patients. Intern J Obstet Anesth 2001; 10: 162–7.
Safa-Tisseront V, Thormann F, Malassine P, et al. Effectiveness of epidural blood patch in the management of post-dural puncture headache. Anesthesiology 2001; 95: 334–9.
Purdie NL, Angle PJ. In vitro validation of 23G epidu-ral catheter performance using standard infusion pump apparatus. Anesthesiology 2004; 101: A36 (abstract).
Angle PJ, Morgan AV, Purdie N. Feasibility study examining the use of 19G epidural needles and 23G epidural catheters for labor analgesia. Anesthesiology 2004; 101: A36 (abstract).
Fleiss JL. Statistical Methods for Rates and Proportions, 2nd ed. New York: Wiley and Sons Publishers; 1981: 14–5.
Halpern S, Preston R. Postdural puncture headache and spinal needle design. Metaanalyses. Anesthesiology 1994; 81: 1376–83.
Holst D, Mollman M, Ebel C, Hausman R, Wendt M. In vitro investigation of cerebrospinal fluid leakage after dural puncture with various spinal needles. Anesth Analg 1998; 87: 1331–5.
Rasmussen BS, Blom L, Hansen P, Mikkelsen SS. Postspinal headache in young and elderly patients. Two randomised, double-blind studies that compared 20-and 25-gauge spinal needles. Anaesthesia 1989; 44: 571–3.
Sage F, Thomas AR, Howard RF. Paediatric lumbar epidurals: a comparison of 21-G and 23-G catheters in patients weighing less than 10 kg. Paediatr Anaesth 2000; 10: 279–82.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Angle, P.J., Hussain, K., Morgan, A. et al. High quality labour analgesia using small gauge epidural needles and catheters. Can J Anesth 53, 263–267 (2006). https://doi.org/10.1007/BF03022213
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03022213