
Abstract
Purpose
To describe the anesthetic management of a patient with previous left lower lobe resection who was submitted to a right upper lobectomy and review the changes in gas exchange and respiratory mechanics which occurred intraoperatively.
Clinical features
A 69-yr-old male with lung cancer, emphysema and obstructive sleep apnea, presented for a right upper lobectomy. His history was also positive for a left lower lobectomy six years previously. Intraoperative lung isolation was achieved using a 41 F left double-lumen tube (DLT). Monitoring the respiratory mechanics allowed for continuous adjustment of ventilator settings during the various phases of the surgery avoiding the risks of barotrauma and volutrauma. Problems with oxygenation occurred during one-lung ventilation.
Conclusion
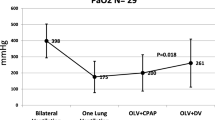
This case report shows that a severe level of hypoxemia and hypercarbia associated to lung mechanical property changes can be observed during the OLV phase. Application of continuous positive airway pressure on the non-dependent lung partially corrected blood oxygenation. Lobe isolation techniques should be considered as useful options for intraoperative airway management for these patients.
Résumé
Objectif
Décrire l’anesthésie d’un patient, ayant déjà subi la résection du lobe inférieur gauche, qui a été soumis à une lobectomie supérieure droite et revoir les changements peropératoires survenus dans les échanges gazeux et la mécanique respiratoire.
Éléments cliniques
Un homme de 69 ans, atteint de cancer du poumon, d’emphysème et d’apnée du sommeil, devait subir une lobectomie supérieure droite. L’isolement pulmonaire peropératoire a été réalisé à l’aide d’un tube 41 Fà double lumière gauche (TDL). Le monitorage de la mécanique respiratoire a permis le réglage continu des paramètres ventilatoires peropératoires et d’éviter les risques de barotrauma et de volutrauma. L’oxygénation a été problématique pendant la ventilation unilatérale (VUL).
Conclusion
Un niveau élevé d’hypoxémie et d’hypercapnie associé à des changements dans les propriétés mécaniques pulmonaires peut être observé pendant la VUL. La ventilation à pression positive constante du poumon non déclive a corrigé partiellement l’oxygénation sanguine. Les techniques d’isolement pulmonaire doivent être envisagées pour la prise en charge peropératoire des voies respiratoires de ce type de patients.
Article PDF
Similar content being viewed by others


References
Ruiz Neto PP. One-lobe ventilation or the hazard of bilateral upper lobectomy (Letter). J Cardiothorac Anesth 1989; 3: 254–5.
Nishimura H,Haniuda M,Morimoto M,Kubo K. Cardiopulmonary function after pulmonary lobectomy in patients with lung cancer. Ann Thorac Surg 1993; 55: 1477–84.
Hagihira S,Maki N,Kawaguchi M,Singer P. Selective bronchial blockage in patients with previous contralateral lung surgery. J Cardiothorac Anesth 2002; 16: 638–42.
Heerdt PM. Cardiovascular adaptation to lung resection.In: Kaplan JA, Slinger PD (Eds). Thoracic Anesthesia, 3rd ed. Philadelphia: Churchill Livingstone Inc.; 2003: 423–35.
Campos JH,Ledet C,Moyers JR. Improvement of arterial oxygen saturation with selective lobar bronchial block during hemorrhage in a patient with previous contralateral lobectomy. Anesth Analg 1995; 81: 1095–6.
Campos JH. Effects on oxygenation during selective lobar versus total lung collapse with or without continous positive airway pressure. Anesth Analg 1997; 85: 583–6.
McGlade DP,Slinger PD. The elective combined use of a double lumen tube and endobronchial blocker to provide selective lobar isolation for lung resection following contralateral lobectomy. Anesthesiology 2003; 99: 1021–2.
Arndt GA,Kranner PW,Rusy DA,Love R. Single-lung ventilation in a critically ill patient using a fiberopti- cally directed wire-guided endobronchial blocker. Anesthesiology 1999; 90: 1484–6.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ruiz, P., Kovarik, G. Lung mechanics and gas exchange in one-lung ventilation following contralateral resection. Can J Anesth 52, 986–989 (2005). https://doi.org/10.1007/BF03022063
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03022063