
Abstract
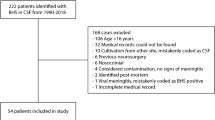
Objective. The aim of this study was to review the clinical features, laboratory findings and the risk factors associated with invasive group A streptococcal infections in children admitted to our institution over a 9-year period (January 1, 1990 through December 31, 1999).Methods: Medical records of children who had a positive blood culture for group A betahemolytic streptococci and children who had this organism isolated from any other sterile site were identified and retrospectively reviewed.Results: Forty-one children with invasive GAS were identified, of whom 15 (36%) were diagnosed between 1990 and 1994, while the balance (26 patients, 63%) were diagnosed between 1995 and 1999 (p< 0.05). The mean age was 4.3 ± 2.5 years (age range: 2 months to 16 years). Thirteen (32%) patients were infants. Sixteen patients had only bacteremia, while 25 patients had in addition to bacteremia the following: cellulitis (n: 13), osteomyelitis (n: 6), pneumonia (n: 3), meningitis (n: 1), pharyngitis (n:3) and Toxic Shock Syndrome (n: 2). Primary varicella infection constituted the most common predisposing factor for invasive GAS infections and occurred in 11 (27%) patients. Leukocytosis (A white blood cell count > 15,000/ mm3) occurred in 21 (51 %) patients, while leukopenia (A white blood cell count < 5000/ mm3) occurred in 2 patients. Parenteral crystalline penicillin G followed by oral penicillin or amoxicillin were the most common antibiotics administered. The mean hospital length of stay was 8 days (range: 6–32 days). All, but one patient survived. The one patient who died had malnutrition and died from streptococcal toxic shock syndrome.Conclusion: More cases of invasive GAS were diagnosed during the second half of the study period, however, the overall rate of occurrence of bacteremia during the study period was consistent with previous reports. Primary varicella infection was the most common predisposing factor for invasive GAS infections. The low occurrence of toxic shock syndrome and fatalities among children with invasive GAS infections are consistent with other pediatric but not with adult series.
Similar content being viewed by others

References
Rathore MH, Barton LL, and Kaplan EL. Suppurative group A beta-hemolytic streptococcal infections in children.Pediatrics 1992; 89: 743–746.
Yagupsky P, Giladi Y. Group A beta-hemolytic streptococcal bacteremia in children.Pediatr Infect Dis J 1987; 6: 1036–1039.
Cone LA, Woodward DR, Schlievert PMet al. Clinical and bacteriologic observations of a toxic shock like syndrome due toStreptococcus pyogenes.N Engl J Med 1987; 317: 146–149.
Wheeler MC, Roe MH, Kaplan ELet al. Severe group A streptococcus septicemia in children. Clinical, epidemiologic, and microbiological correlates.JAMA 1991; 266: 533–437.
Hodge CW, Schwartz B, Talkington DFet al. The changing epidemiology of invasive group A streptococcal infections and the emergence of streptococcal toxic shock-like syndrome. A retrospective population-based study.JAMA 1993; 269: 384–389.
Davies HD, Matlow A, Scriver SRet al. Apparent lower rates of streptococcal toxic shock syndrome and lower mortality in children with invasive group A streptococcal infections compared to adults.Pediatr Infect Dis J 1994; 13: 49–56.
Davies HD, McGeer A, Schwartz Bet al. Invasive group A streptococcal infections in Ontario, Canada. Ontario Group A Streptococcal Study Group.N Eng J Med 1996; 335: 547–554.
Givner L, Abramson J, Wasilauskas B. Apparent increase in the incidence of Group A beta-hemolyric streptococcal disease in children.J Pediatr 1991; 1: 341–346.
Christie C, Havens P, Shapiro E. Bacteremia with group A streptococci in childhood.Am J Dis Child 1988; 142: 559–561.
Belani K, Schlievert P, Kaplan Eet al. Association of exotoxinproducing Group A streptococci and severe disease in children.Peditr Infect Dis J 1991; 10: 351–354.
Jackson M, Burry V, Olson L. Multisystem Group A betahemolytic streptococcal disease in children.Rev Infect Dis 1991; 13: 783–788.
Torres-Martinez C, Mehta D, Butt A, Levin M. Streptococcus associated toxic shock.Arch Dis Child 1992; 67: 126–130.
Stromberg A, Romanus V, Burman L. Outbreak of Group A streptococcal bacteremia in Sweden: an epidemiologic and clinical study.J Infect Dis 1991; 164: 595–598.
Wong V, Wright H. Group A beta hemolytic streptococci as a cause of bacteremia in children.Am J Dis Child 1988;142: 831–833.
Francis J, Warren R. Streptococcus pyogenes bacteremia in Cambridge: a review of 67 episodes.Q J Med 1988; 68: 603–613.
The working Group on prevention of Invasive Group A Streptococcal infections. Prevention of Invasive Group A Streptococcal disease among household contacts of case patients.JAMA 1998; 279: 1206–1210.
Schlieveret PH, Assimacopoulos AP, Cleary PP. Severe invasive group A streptococcal disease: Clinical description and mechanisms of pathogenesis.J Lab Clin Med 1996; 127: 13–22.
Demers B, Simor A, Vellend Het al. Severe invasive Group A streptococcal infections in Ontario, Canada;1987–1991.Clinic Infect Dis 1993; 16: 792–800.
Katz A, Morens D. Severe streptococcal infections in historical perspectives.Clin Infect Dis 1992; 22:421–429.
Bradley JS, Shlievert PM, Sample TG. Streptococcal toxic shock-like syndrome as a complication of varicella.Pediatr Infect Dis J 1991; 10: 77–79
Harnden A, Lennon D. Serious suppurative Group A streptococcal infections in previously well children.Pediatr Infect Dis J 1988; 7: 714–718.
Ferrieri P, Dajani A, Wannamaker L, Chapman S. Natural history of impetigo: 1. Site sequence of acquisition and familial patterns of spread of cutaneous streptococci.J Clin Invest 1972; 51: 2851–2862.
Peterson JL, Vugia DJ, Meyers HBet al. Risk factors for group A streptococcal infections in children with varicella: A casecontrol study.Pediatr Infect Dis J 1996; 15: 151–156.
Doctor A, Harper MB, Fleisher GR. Group A beta hemolytic streptococcal bacteremia: Historical overview, changing incidence, and a recent association with varicella.Pediatrics 1995; 96: 428–433.
Givner LB. Invasive disease due to group A beta-hemolytic streptococci: continued occurrence in children in North Carolina.South Med J 1998; 91: 333–337.
Committee on Infectious Diseases: Recommendations for the use of live attenuated varicella vaccine.Pediatrics 1995; 95: 791–796.
Ibia EO, Imoisili M, Pikis A. Group A beta-hemolyitc streptococcal osteomyelitis in children.Pediatrics 2003; 112: e22-e26. URL: http://www.pediatrics.org/cgi/content/full/112/1/e22.
Gutman L. Osteomyelitis and supurative arthritis. In Katz SL, Gershon AA, Hotez PJ, eds.Krugman’s Infectious Disease of Children. 10th edn. St. Louis, MO: Mosby-Year Book Inc; 1998: 290–301.
Kain Z, Frogel M, Krilov LR. Osteomyelitis associated with varicella infection.Pediatr Infect Dis J 1989; 473–475.
Fischbacher CM, Green ST. Varicella and life-threatening streptococcal infection.Scand J Infect Dis 1987; 19: 519–520.
Stevens D, Tanner M, Winship Jet al. Severe Group A streptococcal infections associated with a toxic shock like syndrome and scarlet fever toxin A.N Engl J Med 1989; 321: 1–4.
Holm S, Norrby A, Bergholm Aet al. Aspects of pathogenesis of serious Group A streptococcal infections in Sweden, 1988–1989.J Infect Dis 1992; 17: 191–195.
Bibler M, Rouan G. Cryptogenic Group A streptococcal bacteremia: experience at an urban general hospital and review of the literature.Rev Infect Dis 1986; 8: 941–951.
Dan M, Maximova S, Siegman-Igra Yet al. Varied clinical presentations of sporadic Group A streptococcal bacteremia: clinical experience and attempt at classification.Rev Infect Dis 1990; 12: 537–542.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Abuhammour, W., Hasan, R.A. & Unuvar, E. Group A Β-Hemolytic streptococcal bacteremia. Indian J Pediatr 71, 915–919 (2004). https://doi.org/10.1007/BF02830836
Issue Date:
DOI: https://doi.org/10.1007/BF02830836