
Abstract
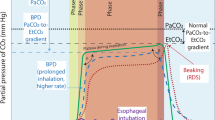
Substantial mean differences between arterial carbon dioxide tension (PaCO2) and end-tidal carbon dioxide tension (PetCO2) in anesthesia and intensive care settings have been demonstrated by a number of investigators. We have explored the technical causes of error in the measurement ofPetCO2 that could contribute to the observed differences. In a clinical setting, the measurement ofPetCO2 is accomplished with one of three types of instruments, infrared analyzers, mass spectrometers, and Raman spectrometers, whose specified accuracies are typically ±2, ±1.5, and ±0.5 mm Hg, respectively. We examined potential errors inPetCO2 measurement with respect to the analyzer, sampling system, environment, and instrument. Various analyzer error sources were measured, including stability, warm-up time, interference from nitrous oxide and oxygen, pressure, noise, and response time. Other error sources, including calibration, resistance in the sample catheter, pressure changes, water vapor, liquid water, and end-tidal detection algorithms, were considered and are discussed. On the basis of our measurements and analysis, we estimate the magnitude of the major potential errors for an uncompensated infrared analyzer as: inaccuracy, 2 mm Hg; resolution, 0.5 mm Hg; noise, 2 mm Hg; instability (12 hours), 3 mm Hg; miscalibration, 1 mm Hg; selectivity (70% nitrous oxide), 6.5 mm Hg; selectivity (100% oxygen), −2.5 mm Hg; atmospheric pressure change, <1 mm Hg; airway pressure at 30 cm H2O, 2 mm Hg; positive end-expiratory pressure or continuous positive airway pressure at 20 cm H2O, 1.5 mm Hg; sampling system resistance, <1 mm Hg; and water vapor, 2.5 mm Hg. In addition to these errors, other systematic mistakes such as an inaccurate end-tidal detection algorithm, poor calibration technique, or liquid water contamination can lead to gross inaccuracies. In a clinical setting, unless the user is confident that all of the technical error sources have been eliminated and the physiologic factors are known, depending onPetCO2 to determine PaCO2 is not advised.
Article PDF
Similar content being viewed by others
Avoid common mistakes on your manuscript.
References
American Society of Anesthesiologists. Standards for basic intraoperative monitoring, House of Delegates of the American Society of Anesthesiologists, October 21, 1986. Park Ridge, IL: American Society of Anesthesiologists, 1986
Zeitlin GL, Cass WA, Gessner JS. Insurance incentives and the use of monitoring devices (letter). Anesthesiology 1988;69:441
Nunn JF, Hill DW. Respiratory dead space and arterial to end-tidal CO2 tension difference in anesthetized man. J Appl Physiol 1960;15:383–389
Whitesell R, Asiddao C, Gollman D, Jablonski J. Relationship between arterial and peak expired carbon dioxide pressure during anesthesia and factors influencing the difference. Anesth Analg 1981;60:508–512
Raemer DR, Francis D, Philip JH, Gabel RA. Variation inPco 2 between arterial blood and peak expired gas during anesthesia. Anesth Analg 1983;62:1065–1069
Epstein MF, Cohen AR, Feldman HA, Raemer DB. Estimation of PaCO2 by two noninvasive methods in the critically ill newborn infant. J Pediatr 1985;106:282–286
Bermudez J, Lichtiger M. Increases in arterial to end-tidal CO2 tension differences after cardiopulmonary bypass. Anesth Analg 1987;66:690–692
Fletcher R. Invasive and noninvasive measurement of the respiratory deadspace in anesthetized children with cardiac disease. Anesth Analg 1988;67:442–447
Gravenstein JS, Paulus DA, Hayes TJ.Capnography in clinical practice. Boston, Butterworths, 1988:103
Raemer DB, Philip JH. Monitoring anesthetic and respiratory gases. In: Blitt CD, ed.Monitoring in anesthesia and critical care medicine. New York, Churchill Livingston, 1989:373–386
Kertzman J. Continuous drying of process sample streams. Paper 73425, Instrument Society of America, Analytical Instrumentation Division, 1973:121–124
Anonymous. Evaluation: carbon dioxide monitors. ECRI Health Dev 1986;15:255–271
Van Wagenen RA, Westenskow DR, Benner RE, et al. Dedicated monitoring of anesthetic and respiratory gases by Raman scattering. J Clin Monit 1986;2:215–222
Ozane GM, Young WG, Mazzei WJ, Severinghaus JW. Multipatient anesthetic mass spectrometry: rapid analysis of data stored in long catheters. Anesthesiology 1981;55:62–70
Severinghaus JW, Young WG. A gas mixer for computer calibration of an anesthetic mass spectrometer. J Clin Monit 1986;2:223–229
Wallace WD, Clark JS, Cutler CA. Blood-gas analyzer calibration and quality control using a precision gas-mixing instrument. Respir Care 1981;26:757–761
Brunner JX, Westenskow DR. How carbon dioxide analyzer rise time affects the accuracy of carbon dioxide measurements (abstr). J Clin Monit 1988;4:134
Westenskow DR, Smith KW, Coleman DL, et al. Clinical evaluation of a Raman scattering multiple gas analyzer for the operating room. Anesthesiology 1989;70:350–355
Weast RC, ed.CRC handbook of chemistry and physics, 58th ed. Cleveland: CRC Press, 1978:F210
Hudson RD.Infrared system engineering. New York: Wiley, 1969
Westenskow DR, Coleman DL. Can the Raman scattering analyzer compete with mass spectrometers: an affirmative reply. J Clin Monit 1989;5:34–36
Severinghaus JW, Larson CP, Eger EI. Correction factors for infrared carbon dioxide pressure broadening by nitrogen, nitrous oxide, and cyclopropane. Anesthesiology 1961;22:429–432
Nielsen JR, Thornton V, Dale EB. The absorption laws for gases in the infra-red. Rev Mod Phys 1944;16:307–324
Epstein RA, Reznick AM, Epstein MAF. Determinants of distortions in CO2 catheter sampling systems: a mathematical model. Respir Physiol 1980;41:127–136
Zupan J, Martin M, Benumof JL. End tidal CO2 excretion waveform and error with gas sampling line leak. Anesth Analg 1988;67:579–581
Severinghaus JW. Water vapor calibration errors in some capnometers: respiratory conventions misunderstood by manufacturers? Anesthesiology 1989;70:996–998
Author information
Authors and Affiliations
Additional information
An erratum to this article is available at http://dx.doi.org/10.1007/BF01619349.
Rights and permissions
About this article
Cite this article
Raemer, D.B., Calalang, I. Accuracy of end-tidal carbon dioxide tension analyzers. J Clin Monitor Comput 7, 195–208 (1991). https://doi.org/10.1007/BF01618124
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01618124