
Abstract
Background
Oral rehydration therapy is the recommended treatment for acute childhood gastroenteritis. The aim of this study was to assess the efficacy and safety of gelatin tannate plus oral rehydration compared with oral rehydration alone.
Methods
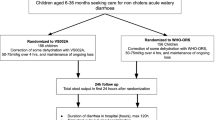
We conducted a multicenter, parallel, randomized, controlled, single-blind, prospective, open-label trial. A central randomization center used computer generated tables to allocate treatments. The study was performed in two medical centers in Italy. Sixty patients 3–72 months of age with acute gastroenteritis were recruited (median age 18 months; age range 3–66 months): 29 received an oral rehydration solution (ORS) and 31 an ORS plus gelatin tannate (ORS + G). The primary outcome was the number of bowel movements 48 and 72 h after initiating treatment. Secondary outcomes were: duration of diarrhea, stool characteristics and adverse events.
Results
No patient was lost at follow-up. No significant difference in the number of bowel movements after 48 h was reported (2.7 ± 1.3 ORS + G; 3.2 ± 0.8 ORS; p = 0.06), although the ORS + G group showed a significant improvement in stool consistency (3.7 ± 1.0 vs. 4.3 ± 0.8; p = 0.005). At 72 h, a significant reduction in bowel movements was reported in the ORS + G group compared with the ORS group (1.0 ± 1.4 vs. 2.0 ± 1.7; p = 0.01). Mean duration of diarrhea was significantly lower in the ORS + G group than in the ORS only group (76.8 ± 19.2 vs. 108 ± 24.0 h; p < 0.0001). No adverse events were reported.
Conclusions
Gelatin tannate added to oral rehydration in children with acute diarrhea was associated with a significant decrease in bowel movements at 72 h, with an early improvement in the stool consistency and shorter disease duration.
Clinical Trial Registration
NCT02644200—Gelatin Tannate as Treatment for Acute Childhood Gastroenteritis (https://www.clinicaltrials.gov).



Similar content being viewed by others


References
Elliott EJ. Acute gastroenteritis in children. BMJ. 2007;6(334):35–40.
Guarino A, Ashkenazi S, Gendrel D, et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition/European Society for Pediatric Infectious Diseases evidence-based guidelines for the management of acute gastroenteritis in children in Europe: update 2014. J Pediatr Gastroenterol Nutr. 2014;59:132–52.
Rahaman MM, Aziz KM, Patwari Y, et al. Diarrhoeal mortality in two Bangladeshi villages with and without community-based oral rehydration therapy. Lancet. 1979;20(2):809–12.
Pollard H, Moreau J, Ronco P, et al. Immunoautoradiographic localisation of enkephalinase (EC 3.4.24.11) in rat gastrointestinal tract. Neuropeptides. 1991;19:169–78.
Szajewska H, Skórka A, Ruszczyński M, et al. Meta-analysis: lactobacillus GG for treating acute gastroenteritis in children-updated analysis of randomised controlled trials. Aliment Pharmacol Ther. 2013;38:467–76.
Lehert P, Chéron G, Calatayud GA, et al. Racecadotril for childhood gastroenteritis: an individual patient data meta-analysis. Dig Liver Dis. 2011;43:707–13.
Das RR, Sankar J, Naik SS. Efficacy and safety of diosmectite in acute childhood diarrhoea: a meta-analysis. Arch Dis Child. 2015;100:704–12.
Farthing M. Novel targets for the pharmacotherapy of diarrhoea: a view for the millennium. J Gastroenterol Hepatol. 2000;15:38–45.
Yoshida T, Amakura Y, Yoshimura M. Structural features and biological properties of ellagitannins in some plant families of the order myrtales. Int J Mol Sci. 2010;11:79–106.
Esteban Carretero J, Durbán Reguera F, López-Argüeta Alvarez S, et al. A comparative analysis of response to ORS (oral rehydration solution) vs ORS + gelatin tannate in two cohorts of pediatric patients with acute diarrhea. Rev Esp Enferm Dig. 2009;101:41–8.
Scaldaferri F, Lopetuso LR, Petito V, et al. Gelatin tannate ameliorates acute colitis in mice by reinforcing mucus layer and modulating gut microbiota composition: emerging role for ‘gut barrier protectors’ in IBD? United European Gastroenterol J. 2014;2:113–22.
Lopetuso LR, Scaldaferri F, Bruno G, et al. The therapeutic management of gut barrier leaking: the emerging role for mucosal barrier protectors. Eur Rev Med Pharmacol Sci. 2015;19:1068–76.
Yoshida T, Amakura Y, Yoshimura M. Structural features and biological properties of ellagitannins in some plant families of the order myrtales. Int J Mol Sci. 2010;11(1):79–106.
Allegrini A, Costantini M. Gelatine tannate for the treatment of acute diarrhoea in adults. J Gastroint Dig Syst. 2012;2:3.
Ruszczyński M, Urbańska M, Szajewska H. Gelatin tannate for treating acute gastroenteritis: a systematic review. Ann Gastroenterol. 2014;27:121–4.
Chumpitazi BP, Lane MM, Czyzewski DI, et al. Creation and initial evaluation of a Stool Form Scale for children. J Pediatr. 2010;157:594–7.
Lane MM, Czyzewski DI, Chumpitazi BP, et al. Reliability and validity of a modified Bristol Stool Form Scale for children. J Pediatr. 2011;159(437–441):e1.
Friedman JN, Goldman RD, Srivastava R, et al. Development of a clinical de-hydration scale for use in children between 1 and 36 months of age. J Pediatr. 2004;145:201–7.
Ashok PK, Upadhyaya K. Tannins are astringent. J Pharmacognosy Phytochem. 2012;1:45–50.
Salazar-Lindo E, Santiesteban-Ponce J, Chea-Woo E, et al. Racecadotril in the treatment of acute watery diarrhea in children. N Engl Med J. 2000;343:463–7.
Strand TA, Sharma PR, Gjessing HK, et al. Risk factors for extended duration of acute diarrhea in young children. PLoS One. 2012;7:e36436.
United Nations Children’s Fund and World Health Organization, ‘WHO/UNICEF Joint Statement: Clinical management of acute diarrhoea’, UNICEF, New York, 2004. http://www.afro.who.int/cah/documents/intervention/acute_diarrhoea_joint_statement.pdf. Accessed June 2009.
Cezard J, Duhamel J, Meyer M, et al. Efficacy and tolerability of Racecadotril in acute diarrhea in children. Gastroenterology. 2001;120(799–805):13.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study protocol was defined in accordance with the Declaration of Helsinki, and was approved by the ethical committee of each participating center (number of protocol 593/12). Written informed consent was obtained from parents of all children.
Conflict of interest
Maurizio Mennini M.D., Carlo Tolone, M.D., Antonella Frassanito M.D., Fabio Midulla M.D. Ph.D., Salvatore Cucchiara M.D. Ph.D. and Marina Aloi M.D., Ph.D. declare that they have no conflict of interest and no financial relationships relevant to this article to disclose.
Funding source
No external funding was received for this manuscript.
Contributors’ statement
Dr. Aloi and Dr Mennini conceptualized and designed the study, drafted the initial manuscript, and approved the final manuscript as submitted. Dr. Tolone and Dr. Mennini allocated and managed enrolled patients. Dr. Aloi and Dr. Frassanito designed the data collection instruments and carried out the initial analyses. Prof. Cucchiara and Prof. Midulla critically reviewed the manuscript and approved the final manuscript as submitted.
Availability of data and materials
Data will not be shared, because of institutional policy. We will, however, be available to share them in the event of a specific request from a reviewer.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Mennini, M., Tolone, C., Frassanito, A. et al. Gelatin Tannate for Acute Childhood Gastroenteritis: A Randomized, Single-Blind Controlled Trial. Pediatr Drugs 19, 131–137 (2017). https://doi.org/10.1007/s40272-016-0207-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40272-016-0207-z