
Abstract
Purpose
Identifying the left ventricular (LV) site associated with the maximum spontaneous interventricular conduction time (right ventricle (RV)-to-LV interval) has proved to be an effective strategy for optimal LV pacing site selection in cardiac resynchronization therapy (CRT). The aim of our study was to determine whether quadripolar LV lead technology allows RV-to-LV interval maximization.
Methods
We enrolled 108 patients undergoing implantation of a CRT system using an LV quadripolar lead and 114 patients who received a bipolar lead. On implantation, the RV-to-LV interval was measured for the dipole of the bipolar leads and for each electrode of the LV lead (tip, ring 2, ring 3, ring 4).
Results
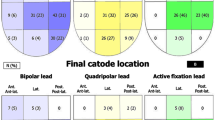
In the quadripolar group, the mean RV-to-LV interval ranged from 90 ± 33 ms (tip) to 94 ± 32 ms (R4) (p > 0.05 for all comparisons). In 55 (51%) patients, the RV-to-LV interval was > 80 ms at all electrodes, while in 27 (25%) patients, no electrodes were associated with an RV-to-LV interval > 80 ms. At least one LV pacing electrode was associated with an RV-to-LV interval > 80 ms in 62 (70%) patients with a short (36 mm) inter-electrode distance, and in 19 (95%, p = 0.022) of those with a long distance (50.5 mm). In the bipolar group, the mean RV-to-LV interval was 72 ± 37 ms (p < 0.001 versus quadripolar). The RV-to-LV interval was > 80 ms in 44 (39%) patients (p < 0.001 versus quadripolar leads with both short and long inter-electrode distance).
Conclusions
Quadripolar leads allow RV-to-LV interval maximization. An optimal RV-to-LV interval seems achievable in the majority of patients, especially if the leads present a long inter-electrode distance.


Similar content being viewed by others

References
Singh JP, Fan D, Heist EK, Alabiad CR, Taub C, Reddy V, et al. Left ventricular lead electrical delay predicts response to cardiac resynchronization therapy. Heart Rhythm. 2006;3:1285–92.
D’Onofrio A, Botto G, Mantica M, La Rosa C, Occhetta E, Verlato R, et al. The interventricular conduction time is associated with response to cardiac resynchronization therapy. Int J Cardiol. 2013;168:5067–8.
Stabile G, D'Onofrio A, Pepi P, De Simone A, Santamaria M, Caico SI, et al. Interlead anatomic and electrical distance predict outcome in CRT patients. Heart Rhythm. 2015;12:2221–9.
Daubert C, Behar N, Martins RP, Mabo P, Leclercq C. Avoiding non-responders to cardiac resynchronization therapy: a practical guide. Eur Heart J. 2016.
Stabile G, Iuliano A, La Rocca V, Solimene F, Fazio R, De Simone A. Geometrical and electrical predictors of cardiac resynchronization therapy response. Expert Rev Cardiovasc Ther. 2014;12:873–84.
Heist EK, Fan D, Mela T, Arzola-Castaner D, Reddy VY, Mansour M, et al. Radiographic left ventricular-right ventricular interlead distance predicts the acute hemodynamic response to cardiac resynchronization therapy. Am J Cardiol. 2005;96:685–90.
Gold MR, Birgersdotter-Green U, Singh JP, Ellenbogen KA, Yu Y, Meyer TE, et al. The relationship between ventricular electrical delay and left ventricular remodelling with cardiac resynchronization therapy. Eur Heart J. 2011;32:2516–24.
Roubicek T, Wichterle D, Kucera P, Nedbal P, Kupec J, Sedlakova J, et al. Left ventricular lead electrical delay is a predictor of mortality in patients with cardiac resynchronization therapy. Circ Arrhythm Electrophysiol. 2015;8:1113–21.
Boriani G, Connors S, Kalarus Z, Lemke B, Mullens W, Osca Asensi J, et al. Cardiac resynchronization therapy with a quadripolar electrode lead decreases complications at 6 months: results of the MORE-CRT Randomized Trial. JACC Clin Electrophysiol. 2016;2:212–20.
Forleo GB, Santini L, Giammaria M, Potenza D, Curnis A, Calabrese V, et al. Multipoint pacing via a quadripolar left-ventricular lead: preliminary results from the Italian registry on multipoint left-ventricular pacing in cardiac resynchronization therapy (IRON-MPP). Europace. .
Philippon F, Liu L, Fung JW, Deharo JC, Anselme F, Delnoy PP, et al. Left ventricular three-dimensional quadripolar lead acute clinical study: the LILAC study. Pacing Clin Electrophysiol. 2015;38:438–47.
Mittal S, Nair D, Padanilam BJ, Ciuffo A, Gupta N, Gallagher P, et al. Performance of anatomically designed quadripolar left ventricular leads: results from the NAVIGATE X4 Clinical Trial. J Cardiovasc Electrophysiol. 2016;27:1199–205.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Roberto Ospizio is an employee of Boston Scientific Italia, no other conflict of interest exists.
Funding
No funding was received.
Rights and permissions
About this article

Cite this article
Stabile, G., Bianchi, V., Solimene, F. et al. Maximization of interventricular conduction time by means of quadripolar leads for cardiac resynchronization therapy. J Interv Card Electrophysiol 50, 111–115 (2017). https://doi.org/10.1007/s10840-017-0279-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-017-0279-x