
Summary
Aim
Arterial hypertension is a serious public health problem because of its frequency and poor management. We compared hypertension control between rural and urban environment over 5 years. Initial hypothesis: arterial pressure control is better in urban (Split) than in rural (Trilj) environment.
Methods
Historic prospective study was conducted in two family medicine outpatient clinics. Data for the years 2005, 2006, and 2010 were analyzed. One hundred and seventeen subjects diagnosed with arterial hypertension in 2005 were examined: 66 in a rural and 51 in urban outpatient clinic. Their average age was 60.92 ± 10.03 (range 30–82 years). Blood pressure records at the onset of the study, the first, and fifth year of treatment, risk factors, and therapy were analyzed. T-test and χ2-test were used in statistical data analysis.
Results
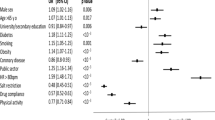
In the urban clinic, more subjects were smokers, had positive family history, were overweight, and had registered hyperlipidemia. Initial mean arterial pressure readings were similar in both the clinics. Decrease was recorded in the following 5 years. During this study the use of ACE inhibitors (ACEI) (Split by 45 %, Trilj by 133 %) and calcium channel blockers (CCB) (Split by 76.9 %, Trilj by 525 %) was increased. The number of patients receiving monotherapy was reduced.
Conclusions
Better arterial pressure control was recorded in the urban clinic, where, after 5 years, despite increased frequency of additional risk factors, the number of normotensive patients was higher than that in the rural one. Hypertension control in both settings was still poor. Hypertensive patients should participate actively in the treatment.
Zusammenfassung
Ziel der Studie
Auf Grund der Häufigkeit und des oft schlechten Managements ist die Hypertonie ein ernstes Problem des öffentlichen Gesundheitswesens. Wir verglichen die Einstellung der Hypertonie über 5 Jahre in einer ländlichen Umgebung mit der einer städtischen. Die anfängliche Hypothese war, dass die Hypertonie- Kontrolle in einer Stadt (Split) besser als am Land (Trilj) sein müsste.
Methodik
In einer historisch-prospektiven Studie wurden die Daten von 2005, 2006 und 2010 zweier Familienpraxen ausgewertet. 117 Patienten (66 aus der ländlichen, 51 aus der städtischen Praxis), bei denen 2005 eine Hypertonie festgestellt worden war, wurden untersucht: das mittlere Alter war 60,92 ± 10,03 (30–82) Jahre. Die RR-Werte vom Beginn der Studie, nach einem Jahr und nach 5 Jahren wurden erhoben. T-Test und χ2-Test wurden zu statistischen Auswertung verwendet.
Ergebnisse
In der städtischen Praxis war die Anzahl der Raucher, der Patienten mit einer positiven Familienanamnese, mit Übergewicht und mit dokumentierter Hyperlipidämie höher. Die initialen RR-Werte waren in beiden Praxen ähnlich. In den folgenden 5 Jahren wurde ein Abfall festgestellt. Während der Studie stieg der Einsatz von ACE-Hemmern (in Split um 45 %, in Trilj um 133 %) und Calciumkanalblocker (in Split um 76,9 %, in Trilj um 525 %). Die Anzahl der Patienten mit Monotherapie wurde reduziert.
Schlussfolgerungen
Die Blutdruckeinstellung war in der städtischen Praxis besser. Nach 5 Jahren war die Zahl der normotensiven Patienten trotz der höheren Häufigkeit von zusätzlichen Risikofaktoren höher als in der Land-Praxis. Die Kontrolle des Hochdrucks war in beiden Praxen noch immer mangelhaft. Patienten mit Hypertonie sollten aktiv an der Behandlung teilnehmen.


Similar content being viewed by others


References
Kannel WB. Blood pressure as a cardiovascular risk factor: prevention and treatment. JAMA. 1996;275:1571–6.
World Health Organization/International Society of Hypertension. 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J Hypertens. 2003;21:1983–92.
Wang KL, Cheng HM, Chuang SY, et al. Central or peripheral systolic or pulse pressure: which best relates to target organs and future mortality? J Hypertens. 2009;27:461–7.
The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). 2007 Guidelines for the management of arterial hypertension. J Hypertens. 2007;25:1105–87.
Simoons ML, Van Der Putten N, Wood D, Boersma E, Bassand JP. The cardiology information system: the need for data standards for integration of systems for patient care, registries and guidelines for clinical practice. Eur Heart J. 2002;23:1148–52.
Zanchetti A, Mancia G, Black HR, et al. Facts and fallacies of blood pressure control in recent trials: implications in the management of patients with hypertension. J. Hypertens. 2009;27:673–9.
Jelaković B, Dika Ž, Kos J, et al. Liječenje i kontrola arterijske hipertenzije u Hrvatskoj (Arterial hypertension treatment and control in Croatia. Summary in English). BEL-AH study. Liječ Vjesn. 2006;128:329–33.
Guidelines Committee. 2003 European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertension. J Hypertens. 2003;21:1011–53.
Pavličević I. Značaj interakcije antihipertenziva i antireumatika u ordinaciji liječnika obiteljske medicine. (Signifiance of antypertensive and antirheumatic drugs in family practice centres. Summary in English). (Doctoral dissertation) Split: Medicinski fakultet Sveučilišta u Splitu; 2009.
Verdecchia P, Staessen JA, Angeli F, et al. Usual versus tight control of systolic blood pressure in nondiabetic patients with hypertension (Cardio-Sis): an open-label randomised trial. Lancet. 2009;374:525–33.
Zanchetti A, Grassi G, Mancia G. When should antihypertensive drug treatment be initiated and to what levels should systolic blood pressure be lowered? A critical reappraisal. J Hypertens. 2009;27:923–34.
Vrhovac B. Interna medicina (Internal medicine). 3rd edition. Zagreb: Naklada ljevak; 2003. pp. 566–84.
Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358:1887–98.
Waeber B, de la Sierra A, Ruilope LM. Target organ damage: how to detect it and how to treat it? J Hypertens. 2009;27 (Suppl 3):13–8.
Paulsena MS, Sondergaarda J, Reutherb L, et al. Treatment of 5413 hypertensive patients: a cross-sectional study. Family Practice. 2011;28(6):599–607.
Stipešević Rakamarić I. Nejednakosti mortaliteta u urbanim i ruralnim sredinama Hrvatske (The uneven mortality rate in urban and rural areas of Croatia. Summary in English) (Magister thesis). Zagreb: Medicinski fakultet Sveučilišta u Zagrebu; 2011.
New Zealand Guidelines Group. New Zealand Primary Care Handbook 2012. 3rd edition Wellington: New Zealand Guidelines Group; 2012.
Krause T, Lovibond K, Caulfield M, McCormack T, Williams B. Management of hypertension: summary of NICE guidance. BMJ. 2011;343:d6255.
Yusuf S, Islam S, Chow CK, et al. Use of secondary prevention drugs for cardiovascular disease in the community in high-income, middle- income, and low-income countries (the PURE Study): a prospective epidemiological survey. The Lancet. 2011;378(9798):1231–43.
Morgan A. A national call to action: CDC’s 2001 urban and rural health chartbook. J Rural Health. 2002;18:382–3
Chang L, McAlister AL, Taylor WC, Chan W. Behavioral change for blood pressure control among urban and rural adults in Taiwan. Health Promot Int. 2003; 18(3):219–28.
Phillips CD, McLeroy KR. Health in rural America: remembering the importance of place. Am J Public Health. 2004;94(10):1661–3.
Murimi MW, Harpel T. Practicing preventive health: the underlying culture among low-income rural populations. J Rural Health. 2010;26(3):273–82.
Jerčić M, Čizmić Z, Vujević M, Puljiz T. Practical training of family medicine in the Dalmatian Hinterland: first hand experience of four physicians. Acta Medica Academica. 2012;41(1):93–9.
Pavličević I. The new curriculum for family medicine at the University of Split School of medicine. Acta Medica Academica. 2012;41(1):26–37.
Yapp CK, Taylor LS, Ow CY, Jamrozik K, Puddey IB. Hypertension management: a comparison of urban versus rural general practitioners in Western Australia. Clin Exp Pharmacol Physiol. 1995;22(6–7):447–9.
Burnier M, Santschi V, Favrat B, Brunner HR. Monitoring compliance in resistant hypertension: an important step in patient management. J Hypertens. 2003;21(Suppl 2):37–42.
Philips LS, Branch WT, Cook BC, et al. Clinical Inertia. Ann Intern Med. 2001;135:825–34.
Conlin PR, Gerth WC, Fox J, Roehm JB, Boccuzzi SJ. Four-year persistence patterns among patients initiating therapy with the angiotensin II receptor antagonist losartan versus other antihypertensive drug classes. Clin Ther. 2001;23:1999–2010.
Ong L K, Cheung BM, May BY, Lau CP, Lam KS. Prevalence, awareness, treatment, and control of hypertension among United States adults 1999–2004. Hypertension. 2007;49:69–75.
Jelaković B, Željković-Vrkić T, Pećin I, et al. Epidemiology of hypertension in Croatia. EHUH study. J Hypertens. 2006;24(4):242.
Wolf-Maier K, Cooper RS, Kramer H. Hypertension treatment and control in 6 European countries, Canada, and the United States. Hypertension. 2004;43:10–7.
Conflict of interest
The authors declare that there is no actual or potential conflict of interest in relation to this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Čikara, A., Pavličević, I. & Perić, I. Level of hypertension control: comparison of a rural and urban family practice centre in South Croatia. Wien Klin Wochenschr 125, 173–179 (2013). https://doi.org/10.1007/s00508-013-0339-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00508-013-0339-x