
Abstract
Purpose
To study the prognostic value of extent, number, and location of positive surgical margins (PSM).
Methods
A total of 1,504 consecutive adjuvant treatment naive and node-negative radical prostatectomy men were included in a prospective database including extent, number, and location of PSM. Mean follow-up was 33 months. Endpoint was biochemical progression-free (bPFS) survival. The impact of margin status and characteristics was assessed in time-dependent analyses using Cox regression and Kaplan–Meier methods.
Results
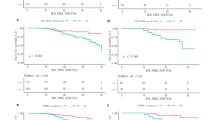
PSM was reported in 26.7 % of patients. The predominant PSM locations were apex and posterior locations. Median PSM length was 4.0 mm. The 2-year bPFS was 73.7 % in PSM patients as compared to 93.0 % in NSM patients (p < 0.001). The rate and extent of PSM increased significantly with pathologic stage (p < 0.001). The extent of PSM length was linearly correlated with bPFS (p = 0.017, coefficient: −0.122). In univariable analysis, extent and number of PSM were significantly linked to outcomes. None of PSM subclassifications significantly influenced the bPFS rates in the subgroup of pT2 disease patients. Conversely, stratification by PSM location (apex vs. other locations, p = 0.008), by PSM number (p = 0.006), and by PSM length (p < 0.001) showed significant differences in pT3-4 cancer patients. In that subgroup, PSM length also added to bPFS prediction using PSM status only in multivariable models (p = 0.005).
Conclusions
PSM subclassifications do not improve the biochemical recurrence prediction in organ-confined disease. In non-organ-confined disease, PSM length (≥3 mm), multifocality (≥3 sites), and apical location are significantly linked to poorer outcomes and could justify a more aggressive adjuvant treatment approach.


Similar content being viewed by others

References
Eastham JA, Kattan MW, Riedel E, Begg CB, Wheeler TM, Gerigk C et al (2003) Variations among individual surgeons in the rate of positive surgical margins in radical prostatectomy specimens. J Urol 170:2292–2295
Fitzsimons NJ, Presti JC Jr, Kane CJ, Terris MK, Aronson WJ, Amling CL et al (2006) Is biopsy Gleason score independently associated with biochemical progression following radical prostatectomy after adjusting for pathological Gleason score? J Urol 176:2453–2458
Hernandez DJ, Epstein JI, Trock BJ, Tsuzuki T, Carter HB, Walsh PC (2005) Radical retropubic prostatectomy. How often do experienced surgeons have positive surgical margins when there is extraprostatic extension in the region of the neurovascular bundle? J Urol 173:446–449
D’Amico AV, Whittington R, Malkowicz SB, Schultz D, Schnall M, Tomaszewski JE et al (1995) A multivariate analysis of clinical and pathological factors that predict for prostate specific antigen failure after radical prostatectomy for prostate cancer. J Urol 154:131–138
Karakiewicz PI, Eastham JA, Graefen M, Cagiannos I, Stricker PD, Klein E et al (2005) Prognostic impact of positive surgical margins in surgically treated prostate cancer: multi-institutional assessment of 5831 patients. Urology 66:1245–1250
Wright JL, Dalkin BL, True LD et al (2010) Positive surgical margins at radical prostatectomy predict prostate cancer specific mortality. J Urol 183:2213–2218
Vis A, Schroder FH, van der Kwast TH (2006) The actual value of the surgical margin status as a predictor of disease progression in men with early prostate cancer. Eur Urol 50:258–265
Freedland SJ, Aronson W, Presti JC Jr et al (2003) Should a positive surgical margin following radical prostatectomy be pathological stage T2 or T3? Results from the SEARCH database. J Urol 169:2142–2161
Salomon L, Anastasiadis AG, Levrel O, Katz R, Saint F, de la Taille A et al (2003) Location of positive surgical margins after retropubic, perineal, and laparoscopic radical prostatectomy for organ-confined prostate cancer. Urology 61:386–390
Stephenson AJ, Wood DP, Kattan MW, Klein EA, Scardino PT, Eastham JA et al (2009) Location, extent and number of positive surgical margins do not improve accuracy of predicting prostate cancer recurrence after radical prostatectomy. J Urol 182:1357–1363
Mauermann J, Fradet V, Lacombe L, Dujardin T, Tiguert R, Tetu B et al (2013) The impact of solitary and multiple positive surgical margins on hard clinical end points in 1712 adjuvant treatment-naive pT2-4 N0 radical prostatectomy patients. Eur Urol 64:19–25
Tan PH, Cheng L, Srigley JR, Griffiths D, Humphrey PA, van der Kwast TH et al (2011) ISUP Prostate Cancer Group. International Society of Urological Pathology (ISUP) Consensus Conference on Handling and Staging of Radical Prostatectomy Specimens. Working group 5: surgical margins. Mod Pathol 24:48–57
Epstein JI, Allsbrook WC Jr, Amin MB, Egevad LL (2005) ISUP Grading Committee. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am J Surg Pathol 29:1228–1242
Udo K, Cronin AM, Carlino LJ, Savage CJ, Maschino AC, Al-Ahmadie HA et al (2013) Prognostic impact of subclassification of radical prostatectomy positive margins by linear extent and Gleason grade. J Urol 189:1302–1307
Sooriakumaran P, Ploumidis A, Nyberg T et al (2013) The impact of length and location of positive margins in predicting biochemical recurrence after robotic-assisted radical prostatectomy with a minimum follow-up time of five years. BJU Int (in press)
d’Amico AV, Whittington R, Malkowicz SB et al (1998) The combination of preoperative prostate specific antigen and postoperative pathological findings to predict prostate specific antigen outcome in clinically localized prostate cancer. J Urol 160:2096–2101
Grossfeld GD, Chang JJ, Broering JM et al (2000) Impact of positive surgical margins on prostate cancer recurrence and the use of secondary cancer treatment: data from the CaPSURE database. J Urol 163:1171–1177
Boorjian SA, Karnes RJ, Crispen PL, Carlson RE, Rangel LJ, Bergstralh EJ, Blute ML (2010) The impact of positive surgical margins on mortality following radical prostatectomy during the prostate specific antigen era. J Urol 183(3):1003–1009
Ohori M, Wheeler TM, Kattan MW, Goto Y, Scardino PT (1995) Prognostic significance of positive surgical margins in radical prostatectomy specimens. J Urol 154:1818–1824
Orvieto MA, Alsikafi NF, Shalhav AL, Laven BA, Steinberg GD, Zagaja GP, Brendler CB (2006) Impact of surgical margin status on long-term cancer control after radical prostatectomy. BJU Int 98:1199–1203
Ploussard G, Agamy MA, Alenda O, Allory Y, Mouracade P, Vordos D et al (2011) Impact of positive surgical margins on prostate-specific antigen failure after radical prostatectomy in adjuvant treatment-naïve patients. BJU Int 107:1748–1754
Porpiglia F, Fiori C, Manfredi M, Grande S, Poggio M, Bollito E et al (2012) Surgical margin status of specimen and oncological outcomes after laparoscopic radical prostatectomy: experience after 400 procedures. World J Urol 30:245–250
Somford DM, van Oort IM, Cosyns JP, Witjes JA, Kiemeney LA, Tombal B (2012) Prognostic relevance of number and bilaterality of positive surgical margins after radical prostatectomy. World J Urol 30:105–110
Eastham JA, Kuroiwa K, Ohori M, Serio AM, Gorbonos A, Maru N et al (2007) Prognostic significance of location of positive margins in radical prostatectomy specimens. Urology 70:965–969
Fesseha T, Sakr W, Grignon D, Banerjee M, Wood DP Jr, Pontes JE (1997) Prognostic implications of a positive apical margin in radical prostatectomy specimens. J Urol 158:2176–2179
Blute ML, Bostwick DG, Bergstralh EJ, Slezak JM, Martin SK, Amling CL et al (1997) Anatomic site-specific positive margins in organ-confined prostate cancer and its impact on outcome after radical prostatectomy. Urology 50:733–739
Bolla M, van Poppel H, Collette L, van Cangh P, Vekemans K, Da Pozzo L et al (2005) Postoperative radiotherapy after radical prostatectomy: a randomised controlled trial (EORTC trial 22911). Lancet 366:572–578
Thompson IM Jr, Tangen CM, Paradelo J, Lucia MS, Miller G, Troyer D et al (2006) Adjuvant radiotherapy for pathologically advanced prostate cancer: a randomized clinical trial. JAMA 296:2329–2335
Wiegel T, Bottke D, Steiner U et al (2009) Phase III postoperative adjuvant radiotherapy after radical prostatectomy compared with radical prostatectomy alone in pT3 prostate cancer with postoperative undetectable prostate-specific antigen: ARO 96-02/AUO AP 09/95. J Clin Oncol 27:2924–2930
Freedland SJ, Humphreys EB, Mangold LA, Eisenberger M, Partin AW (2006) Time to prostate specific antigen recurrence after radical prostatectomy and risk of prostate cancer specific mortality. J Urol 176:1404–1408
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Guillaume Ploussard and Sarah J. Drouin have contributed equally to this work.
Rights and permissions
About this article
Cite this article
Ploussard, G., Drouin, S.J., Rode, J. et al. Location, extent, and multifocality of positive surgical margins for biochemical recurrence prediction after radical prostatectomy. World J Urol 32, 1393–1400 (2014). https://doi.org/10.1007/s00345-014-1243-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-014-1243-3