
Summary
Conclusion
Congenital aplasia of the body and tail of the pancreas is derived from a defect of the dorsal pancreatic anlage and should not be considered a type of acquired atrophy of these structures.
Background
Congenital aplasia of the body and tail of the pancreas radiologically mimics acquired atrophy of the pancreatic body and tail.
Methods
Two patients with radiologically identified aplasia of the body and tail of the pancreas were studied clinicopathologically.
Results
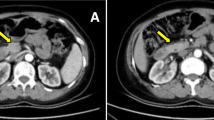
An 82-yr-old man was diagnosed radiologically as having both carcinoma of the head of the pancreas and aplasia of the body and tail of the pancreas and underwent pancreatoduodenectomy. Pathologically the carcinoma was distributed in the anterosuperior part of the head of the pancreas, and spread into the duct of Santorini and intraductally to a portion of the main pancreatic duct beyond the junction of the ducts of Santorini and Wirsung. Consequently, obstructive pancreatitis of the body and tail of the pancreas developed, resulting in marked atrophy that mimicked aplasia of the body and tail of the pancreas. A 74-yr-old woman was diagnosed radiologically as having two carcinomas, one of the gallbladder and one of the stomach, and aplasia of the body and tail of the pancreas. During surgery, suspected parenchymal disappearance and fatty replacement in the body and tail of the pancreas were noted. Histologic examination of biopsy specimens from the body portion revealed atrophic pancreatic tissue surrounded by fat. Therefore, these patients had atrophy of the pancreatic body and tail.
Similar content being viewed by others


References
Heiberg KA. Ein Fall von fehlender Cauda pancreatic (bei einem Diabetiker).Zentralbl Allg Pathol 1911; 22: 676,677.
Ghon A, Roman B. Ein Fall von Missbildung des Pankreas mit Diabetes mellitus.Prag Med Wochenschr Nr 1913; 38: 524–526.
Christlieb. Angeborenes Fehlen von Bauchspeichel-drüsenteilen mit ausgleichender Vergrösserung und Vermekrung der Langerhansschen Inseln.Virchows Arch [A] 1933; 289: 241–246.
Duschl L. Ein Beitrag zu den Pankreasmissbildungen: Fehlen des Pancreaskopfes und-schwanzes.Münchener Medizinische Wochenschrift 1923; 70: 1388,1389.
Priesel A. Funf Falle von Bildungs-anomalien des Pankreas (reported in Vereinigung der Pathologischen Anatomen Wiens).Wiener Klinishe Wochenschrift Nr 1923; 22: 407.
Smetana H. Ein Beitrag zur Kenntnis der Missbildungen des Pankreas.Path Anat 1928; 80: 239–256.
Akazaki K. Ein Beitrag zur Pankreas hypoplasie mit Coma diabeticum.Tokyo Igakukkai Zasshi 1934; 48: 1842–1851
Lechner GW, Read RC. Agenesis of the dorsal pancreas in an adult diabetic presenting with duodenal ileus.Ann Surg 1966; 163: 311–314.
Suda K, Mizuguchi K, Hoshino A. Differences of the ventral and dorsal anlagen of pancreas after fusion.Acta Pathol Jpn 1981; 31: 583–589.
Morita M, Otsubo T, Kozu T, Shibata I, Toki F, Oi I, Takeuchi T, Takada T, Nakamura K, Harnano K, Kobayashi S, Hanyu F. Aplasia of body and tail of the pancreas: a report of two cases.Jpn J Gastroenterol 1980; 77: 102–106.
Kloppel G, Lenzen S. Anatomy and physiology of the endocrine pancreas, inPancreatic Pathology, Klöppel G, Heitz FL, eds. Churchill Livingstone, New York 1984; pp. 133–153.
Suda K, Yuminamochi T, Ishii Y, Nakazawa K, Oyarna T, Kawaoi A. Distribution of endocrine cells based on difference of the pancreatic anlagen.Jap J Clin Pathol 1987; 35: 809–812.
Yokota T, Mizumoto R, Honjo I. Fatty metamorphosis of distal pancreas with tumors in preampullary region—report of 3 cases.Saishin Igaku 1975; 30: 2247–2250.
Cohen DJ, Fagelman O. Pancreas islet cell carcinoma with complete fatty replacement: CT characteristics.J Comput Assist Tomog 1986; 10: 1050,1051.
Suda K, Mogaki M, Oyama I, Matsumoto Y. Histopathological and immunohistochemical studies on alcoholic pancreatitis and chronic obstructive pancreatitis: special emphasis on ductal obstruction and genesis of pancreatitis.Am J Gastroenterol 1990; 85: 271–276.
Cotton PB, Kizu M. Malfusion of dorsal and ventral pancreas. A cause of pancreatitis?Gut 1977; 18: 400 (abstract).
Suda K, Hirai S, Yamamura A, Itakura J, Matsumoto Y, Sato K, Ariyama J. A histopathological study on ventral and dorsal pancreas in patients with pancreas divisum.Dig Endosc 1994; 6: 74–79.
Author information
Authors and Affiliations
Additional information
An erratum to this article is available at http://dx.doi.org/10.1007/BF02925975.
Rights and permissions
About this article
Cite this article
Suda, K., Matsumoto, Y., Fujii, H. et al. Clinicopathologic differentiation of atrophy of the pancreatic body and tail aplasia. Int J Pancreatol 24, 227–235 (1998). https://doi.org/10.1007/BF02788426
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02788426