
Abstract
Acute exacerbation of idiopathic pulmonary fibrosis (IPF) is a clinically important complication of IPF that carries a high morbidity and mortality. In the last decade, we have learned much about this event, but there are many remaining questions: What is it? Why does it happen? How can we prevent it? How can we treat it? This chapter attempts to summarize our current understanding of the epidemiology, etiology, and management of acute exacerbation of IPF and point out areas where additional data are sorely needed.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
A Case
A 78-year-old man was referred for surgical lung biopsy in the evaluation of his interstitial lung disease (ILD). At baseline, he reported mild dyspnea on exertion and a chronic, dry cough. His past medical history was significant for hypertension and gastroesophageal reflux (GER) disease. His medications included an antihypertensive medication and a proton pump inhibitor. He was a lifelong nonsmoker and worked as a dentist. He had no family history of ILD. His physical exam was significant for dry inspiratory crackles at both bases and normal resting oxygen saturation. His pulmonary function was abnormal with a forced vital capacity of 57 % predicted and a diffusing capacity for carbon monoxide of 67 % predicted. His high-resolution computed tomography (HRCT) scan demonstrated peripheral, subpleural predominant reticulation and traction bronchiectasis without honeycombing.
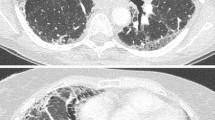
He was referred for surgical lung biopsy and had a video-assisted thoracic surgery procedure with biopsies obtained from the right lung. His perioperative course was uncomplicated. His pathology was reviewed and was consistent with a usual interstitial pneumonia (UIP) pattern, confirming the diagnosis of IPF. His initial postoperative course was uncomplicated, but approximately 5 days postoperatively, he developed increased dyspnea and cough with occasional production of clear sputum. He had new-onset hypoxemia (88 % on room air) with diffuse crackles to auscultation that were more prominent in the left chest. A repeat HRCT demonstrated new ground-glass opacities in the left lung (Fig. 17.1). All microbiologic data were negative, and there was no evidence of cardiac dysfunction or ischemia.

Bottom left image is presurgery demonstrating peripheral reticulation and traction bronchiectasis without honeycombing. Upper right image is 5 days postoperatively, demonstrating diffuse ground-glass opacities, most prominent in the left lung
This case was thought to be due to an acute exacerbation (AEx) of IPF triggered by surgical lung biopsy possibly due to single lung ventilation of the left lung. Unfortunately, the patient progressively worsened despite supportive care and subsequently died from his AEx of IPF.
Epidemiology, Clinical Features, and Risk Factors
Our view of the natural history of IPF has changed over the last decade with the recognition that there are several distinct clinical courses that patients may follow [1]. Although most patients with IPF experience a steady decline in lung function over time, some will decline quickly, while others seem stable for many years. Increasingly, we recognize that some patients may also have a more unpredictable course [2]. These patients experience periods of relative stability followed by acute episodes of worsening in their respiratory status [3]. Episodes of acute respiratory decline in IPF can be secondary to complications such as infection, pulmonary embolism, pneumothorax, or heart failure [3, 4]. Such episodes of acute respiratory deterioration have been termed AEx of IPF when the cause for the acute worsening cannot be identified. Acute exacerbations likely comprise almost 50 % of these acute respiratory events, and the clinical characteristics and prognosis are indistinguishable from acute exacerbations of known cause. This chapter will discuss only AEx of IPF.
The phenomenon of AEx has been recognized since the late 1980s, when it was initially reported in the Japanese literature [5–8]. A survey of providers in the USA suggests that most clinicians believe AEx to be somewhat or very common [9]. The true incidence of AEx remains unknown, and the incidence may vary by country due to different genetic and environmental factors. Largely due to differences in case definition, patient population, sample size, and duration of follow-up, the range of AEx incidence in clinical studies ranges anywhere from 1 % to 24 % [3, 4]. The largest and probably most robust study of 461 patients with IPF that were followed longitudinally over 3 years found a 1- and 3-year incidence of 14.2 % and 20.7 %, respectively [4].
The clinical presentation of AEx is generally quite dramatic and characterized by acute to subacute worsening of dyspnea over days to weeks [3]. Some patients experience symptoms of worsening cough, sputum production, and fever mimicking a respiratory tract infection [10, 11]. Most reported cases of AEx have required unscheduled medical attention (emergency room or hospital care), but there may well be less severe cases that do not get noted by patients and providers and, therefore, are not documented.
The occurrence of AEx is unpredictable and can sometimes be the presenting manifestation of IPF [11–13]. A few risk factors have been identified, including lower baseline forced vital capacity (FVC) % predicted and having been a nonsmoker [4]. It seems likely that patients with more severe IPF are more likely to develop clinically significant AEx of disease, and this perception is supported by the increased incidence of AEx that was observed in the only study of advanced disease reported in the literature to date, namely, STEP-IPF [14]. Precipitating factors such as surgical lung biopsy and bronchoalveolar lavage (BAL) have also been reported [11, 15–20]. The occurrence of AEx after videoscopic-assisted surgical lung biopsy is particularly intriguing, as the exacerbation appears to be more pronounced in the lung that was ventilated (i.e., the nonsurgical side receiving single lung ventilation) [19]. However, the precise relationship between these precipitating factors and AEx remains unclear.
Acute exacerbations have also been described in non-IPF ILD, including nonspecific interstitial pneumonia (NSIP) [21], connective tissue disease-associated ILD [21–23], and hypersensitivity pneumonitis [24, 25]. Compared to IPF AEx, patients with an underlying NSIP pattern appeared to have a better prognosis following their AEx [21]. A UIP pattern may be a risk factor for AEx in the context of connective tissue disease-associated ILD and hypersensitivity pneumonitis, as the presence of a UIP pattern appeared to be a risk factor in some case series [21, 25]. Whether AEx of non-IPF forms of ILD shares a similar pathobiology as AEx of IPF is unknown.
Etiology and Pathobiology
The etiology of AEx of IPF remains unknown. Several hypotheses have been proposed, including the following: (1) AEx of IPF represents an abrupt acceleration of the patients underlying disease; (2) AEx is a collection of occult, pathobiologically distinct conditions (e.g., infection, heart failure); or (3) AEx is a combination of both processes that can serve as an occult trigger that leads to acceleration of the underlying fibroproliferative process.
Occult aspiration of gastric contents has been suggested as a possible trigger or cause of AEx of IPF. GER is nearly universal in patients with IPF [26, 27] and is thought to be a risk factor for aspiration [28, 29]. BAL pepsin levels, a biomarker for aspiration of gastric secretions, were shown to be elevated in a subset of patients with AEx of IPF [30]. In addition, patients with asymmetric IPF on HRCT scan had a higher rate of GER and AEx compared to patients with non-asymmetric disease, suggesting a role for GER and occult aspiration in a subset of patients with IPF [31].
Infection has also been suggested as a cause of AEx of IPF. Data in support of this hypothesis include animal studies [32] as well as some human studies [33, 34]. In one case series, 75.7 % of 37 AEx cases occurred between December and May [10], lending further support to occult infection as a cause of AEx. However, in a prospective study of AEx of IPF (n = 47), acute viral infection, as determined by the most current genomics-based methodologies, was found in only 9 % of this cohort [35]. While some cases may well have been missed (i.e., the virus had come and gone by the time testing was obtained), these data suggest that there are many cases of AEx that are not primarily due to occult infection.
An alternative explanation is that AEx of IPF is caused by an inherent acceleration of the pathobiology of IPF [3]. There is indirect evidence for this in several studies that evaluated serum biomarkers and gene expression in AEx. Serum biomarkers of alveolar epithelial cell injury/proliferation have been shown to be increased in AEx, in a pattern that is qualitatively distinct from what is seen in acute lung injury (Table 17.1).
Gene expression studies performed in patients with AEx of IPF [37] have shown that patients have increased expression of genes encoding proteins involved in epithelial injury and proliferation including CCNA2 and alpha-defensins. Interestingly, there was no evidence from the same study for upregulation of genes commonly expressed in viral infection.
Work-Up and Diagnostic Criteria
Laboratory Evaluation
There are no specific laboratory tests that aid in the evaluation and diagnosis of AEx of IPF. Often, patients are found to have impaired gas exchange with a decrease in their arterial oxygen tension [10]. In patients that can tolerate bronchoscopy with lavage, an increase in BAL neutrophils has been reported [11, 45]. Nonspecific elevations in serum lactate dehydrogenase (LDH) and C-reactive protein (CRP) have also been observed [10]. Serial levels of serum KL-6 and baseline thrombomodulin may help identify patients at increased risk for death from AEx [42, 43]. Although many experimental biomarkers have been investigated, as shown in Table 17.1, none are routinely used in clinical practice.
Radiologic Evaluation
High-resolution CT scans are often obtained during AEx of IPF. The findings include new, generally bilateral, ground-glass opacities and/or consolidation superimposed on the underlying UIP pattern [46]. The pattern of ground-glass changes during an AEx may have prognostic significance, with more diffuse abnormality correlating with worse outcomes [46].
Histopathologic Evaluation
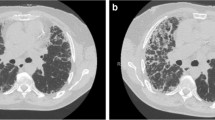
Surgical lung biopsy is not frequently obtained during AEx of IPF. A small case series of seven patients who had a surgical lung biopsy during their AEx demonstrated primarily diffuse alveolar damage (DAD) associated with underlying changes typical for UIP (Fig. 17.2) [47]. One case had organizing pneumonia and UIP and another case had DAD without underlying UIP. Autopsy series and other case series have demonstrated similar findings [6, 11, 45, 48–50].

Section from lung explant shows subpleural fibrosis with honeycombing typical of usual interstitial pneumonia. The central lung tissue shows diffuse alveolar septal thickening by edema and type II pneumocyte hyperplasia, and airspace consolidation by edema and fibrin (H&E, ×100). Figure courtesy of Kirk Jones, MD
Diagnostic Criteria
Several definitions have been used over the last decade to define AEx of IPF [3, 6, 50]. In order to standardize these criteria, a consensus definition was proposed by the National Institutes of Health-funded US IPF Network (IPFNet) in 2007 (Table 17.2) [3]. Other definitions that have been described are generally similar; however, they often include a reduction in PaO2 as one of their criteria as well as bilateral chest x-ray abnormalities (instead of a HRCT scan) [6, 50].
The IPFNet criteria have helped to standardize the definition of AEx of IPF, but satisfaction of all criteria is quite difficult to achieve in many clinical settings. Specifically, it is not infrequent that in patients who appear to have AEx of IPF, microbiologic data and occasionally radiologic data are not collected due to the severity of illness or because the clinician does not feel the tests will change clinical management. By maximizing specificity at the cost of sensitivity, these criteria (along with the selection of only mild to moderate patients for enrollment) have likely contributed to the low prevalence of AEx observed in recent clinical trials [51–53]. The choice of definition has significant implications for outcome analyses in clinical trials and should be a focus for further discussion among clinical trialists.
Management and Prognosis
There is no known effective treatment for preventing or improving outcomes in AEx of IPF.
Prevention
While there are no data to support efficacy, vaccination and treatment of comorbidities like heart disease and GER seem prudent as measures that could prevent episodes of acute decline in respiratory function due to known causes such as infection, heart failure, and aspiration. Some novel therapies have suggested a reduction in AEx in clinical trials; these include warfarin [54], pirfenidone [55], and, most recently, BIBF 1120 [56]. Unfortunately, both warfarin and pirfenidone have subsequently been shown to have no impact on the rate of AEx, suggesting that the initial observations were inaccurate [51, 57].
Medical Therapy During AEx
Although commonly prescribed for the treatment of AEx of IPF, there have been no controlled trials assessing the efficacy of high-dose corticosteroids. Recent international guidelines on IPF management suggested that the majority of IPF patients with AEx could be treated with corticosteroids [58]; however, approaches to dosing, route, and duration of therapy were not provided.
Although most clinicians would treat patients who develop an AEx of IPF with high-dose corticosteroids, the efficacy of this treatment is unclear. Perhaps we should be more critical of the use of corticosteroids to treat AEx of IPF. There are two distinct viewpoints regarding the role of corticosteroids in AEx of IPF. The first viewpoint is that AEx of IPF is histopathologically similar to acute respiratory distress syndrome (ARDS) characterized by DAD and acute lung injury [59] and should, therefore, be treated similarly to ARDS. In the ARDS literature, the mortality benefit of corticosteroids is unclear [60–65]. In one study, increased mortality was observed in ARDS patients treated with delayed corticosteroids (after 14 days) [65]. If we were to follow the ARDS paradigm, most clinicians would not use corticosteroids in the treatment of AEx of IPF. A second viewpoint for the role of corticosteroids in IPF is that some patients with AEx of IPF have organizing pneumonia on biopsy [49]. Organizing pneumonia is generally thought to be steroid responsive, and it may be that the pathobiology is different enough between ARDS and AEx of IPF to warrant continued use of corticosteroids. There remains equipoise on the efficacy of corticosteroids in AEx of IPF, and this treatment intervention should be studied more carefully [42].
The use of another immunosuppressant, cyclosporine A, to treat AEx of IPF has been reported. These studies suggest some benefit to the use of cyclosporine A plus corticosteroids [66–68]. However, conclusions that can be made from these data are limited by problems with study design and small sample size, and benefit has not yet been validated in a randomized controlled trial.
Other experimental therapies that have reported possible efficacy to treat AEx of IPF include tacrolimus [69], hemoperfusion with polymyxin B-immobilized fiber column [70–72], and sivelestat [73]. These investigations were all limited by small numbers and suboptimal study design.
Supportive Therapy During AEx
Supportive therapy is the standard of care in AEx of IPF. Supportive care for respiratory failure almost always requires higher oxygen supplementation and consideration of additional means of ventilatory support, including mechanical ventilation (see discussion below) and noninvasive positive-pressure ventilation (NIPPV). Yokoyama et al. described the outcomes of patients with AEx of IPF treated with NIPPV to avoid intubation in acute respiratory failure [74]. In this retrospective case series of 11 patients, 6 patients failed a NIPPV trial and went subsequently succumbed to respiratory failure. The other five patients survived more than 3 months after the onset of their AEx. However, the use of ventilatory support in AEx (both mechanical ventilation and NIPPV) has never been studied in a randomized controlled trial.
Lung Transplantation
A few select centers have experience with emergent transplantation for AEx of IPF [75–78]. These critically ill IPF patients have generally been bridged to lung transplant with extracorporeal membrane oxygenation (ECMO) and/or mechanical ventilation [76]. Outcomes of patients who have undergone emergent transplantation have been mixed [77, 78]. Emergent lung transplantation requires careful patient selection and is not done at all transplant centers.
Prognosis
The prognosis of AEx of IPF is poor, with most case series reporting very high short-term mortality rates [11, 79–83]. This is particularly true for those patients requiring mechanical ventilation. A systematic review of mechanical ventilation in IPF and respiratory failure (n = 135), including AEx, reported a hospital mortality of 87 % [81]. Short-term mortality (within 3 months of hospital discharge) was 94 %. The routine use of mechanical ventilation in patients with AEx of IPF is not recommended in the international consensus guidelines because of its low likelihood of benefit and high risk of complications and further suffering [58]. Careful consideration regarding intubation and goals of care must be made, given the poor prognosis associated with this condition. Ideally, a discussion concerning end-of-life issues should be held between the patient and their provider in the outpatient setting with the inclusion of the patient’s family, if applicable.
Summary
Acute exacerbation of IPF is responsible for substantial morbidity and mortality in patients with IPF. We suggest that AEx of IPF represents an acute acceleration of the fibroproliferative process (i.e., the underlying pathobiology of IPF) that is triggered by some generally occult stress or insult to the lung (e.g., infection, aspiration, mechanical stretch from ventilation or lavage, high inspired oxygen concentration during surgery). As many patients with AEx of IPF will not meet the current consensus criteria due to missing data, it may be more useful clinically to define AEx by less stringent criteria. It seems likely that the prevention and treatment of AEx of IPF must focus on both disease-specific (e.g., anti-fibrotic therapies) and non-disease-specific (e.g., vaccination, prevention of stress) areas. The next decade will hopefully answer many of the unresolved questions concerning AEx of IPF.
References
Kim DS, Collard HR, King Jr TE. Classification and natural history of the idiopathic interstitial pneumonias. Proc Am Thorac Soc. 2006;3(4):285–92.
Ley B, Collard HR, King Jr TE. Clinical course and prediction of survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;183(4):431–40.
Collard HR, Moore BB, Flaherty KR, Brown KK, Kaner RJ, King Jr TE, et al. Acute exacerbations of idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2007;176(7):636–43.
Song JW, Hong SB, Lim CM, Koh Y, Kim DS. Acute exacerbation of idiopathic pulmonary fibrosis: incidence, risk factors and outcome. Eur Respir J. 2011;37(2):356–63.
Suga T, Sugiyama Y, Ohno S, Kitamura S. [Two cases of IIP which developed acute exacerbation after bronchoalveolar lavage]. Nihon Kyobu Shikkan Gakkai Zasshi. 1994;32(2):174–8.
Kondoh Y, Taniguchi H, Kawabata Y, Yokoi T, Suzuki K, Takagi K. Acute exacerbation in idiopathic pulmonary fibrosis. Analysis of clinical and pathologic findings in three cases. Chest. 1993;103(6):1808–12.
Kondo A, Saiki S. Acute exacerbation in idiopathic interstitial pneumonia (IIP). In: Harasawa M, Fukuchi Y, Morinari H, editors. Interstitial pneumonia of unknown etiology. Tokyo: University of Tokyo Press; 1989.
Horio H, Nomori H, Morinaga S, Fuyuno G, Kobayashi R, Iga R. [Exacerbation of idiopathic interstitial pneumonia after lobectomy for lung cancer]. Nihon Kyobu Shikkan Gakkai Zasshi. 1996;34(4):439–43.
Collard HR, Loyd JE, King Jr TE, Lancaster LH. Current diagnosis and management of idiopathic pulmonary fibrosis: a survey of academic physicians. Respir Med. 2007;101(9):2011–6.
Simon-Blancal V, Freynet O, Nunes H, Bouvry D, Naggara N, Brillet PY, et al. Acute exacerbation of idiopathic pulmonary fibrosis: outcome and prognostic factors. Respiration. 2012;83(1):28–35.
Kim DS, Park JH, Park BK, Lee JS, Nicholson AG, Colby T. Acute exacerbation of idiopathic pulmonary fibrosis: frequency and clinical features. Eur Respir J. 2006;27(1):143–50.
Sakamoto K, Taniguchi H, Kondoh Y, Ono K, Hasegawa Y, Kitaichi M. Acute exacerbation of idiopathic pulmonary fibrosis as the initial presentation of the disease. Eur Respir Rev. 2009;18(112):129–32.
Kondoh Y, Taniguchi H, Katsuta T, Kataoka K, Kimura T, Nishiyama O, et al. Risk factors of acute exacerbation of idiopathic pulmonary fibrosis. Sarcoidosis Vasc Diffuse Lung Dis. 2010;27(2):103–10.
Zisman DA, Schwarz M, Anstrom KJ, Collard HR, Flaherty KR, Hunninghake GW. A controlled trial of sildenafil in advanced idiopathic pulmonary fibrosis. N Engl J Med. 2010;363(7):620–8.
Zegdi R, Azorin J, Tremblay B, Destable MD, Lajos PS, Valeyre D. Videothoracoscopic lung biopsy in diffuse infiltrative lung diseases: a 5-year surgical experience. Ann Thorac Surg. 1998;66(4):1170–3.
Yuksel M, Ozyurtkan MO, Bostanci K, Ahiskali R, Kodalli N. Acute exacerbation of interstitial fibrosis after pulmonary resection. Ann Thorac Surg. 2006;82(1):336–8.
Utz JP, Ryu JH, Douglas WW, Hartman TE, Tazelaar HD, Myers JL, et al. High short-term mortality following lung biopsy for usual interstitial pneumonia. Eur Respir J. 2001;17(2):175–9.
Kumar P, Goldstraw P, Yamada K, Nicholson AG, Wells AU, Hansell DM, et al. Pulmonary fibrosis and lung cancer: risk and benefit analysis of pulmonary resection. J Thorac Cardiovasc Surg. 2003;125(6):1321–7.
Kondoh Y, Taniguchi H, Kitaichi M, Yokoi T, Johkoh T, Oishi T, et al. Acute exacerbation of interstitial pneumonia following surgical lung biopsy. Respir Med. 2006;100(10):1753–9.
Hiwatari N, Shimura S, Takishima T, Shirato K. Bronchoalveolar lavage as a possible cause of acute exacerbation in idiopathic pulmonary fibrosis patients. Tohoku J Exp Med. 1994;174(4):379–86.
Park IN, Kim DS, Shim TS, Lim CM, Lee SD, Koh Y, et al. Acute exacerbation of interstitial pneumonia other than idiopathic pulmonary fibrosis. Chest. 2007;132(1):214–20.
Tachikawa R, Tomii K, Ueda H, Nagata K, Nanjo S, Sakurai A, et al. Clinical features and outcome of acute exacerbation of interstitial pneumonia: collagen vascular diseases-related versus idiopathic. Respiration. 2012;83(1):20–7.
Suda T, Kaida Y, Nakamura Y, Enomoto N, Fujisawa T, Imokawa S, et al. Acute exacerbation of interstitial pneumonia associated with collagen vascular diseases. Respir Med. 2009;103(6):846–53.
Olson AL, Huie TJ, Groshong SD, Cosgrove GP, Janssen WJ, Schwarz MI, et al. Acute exacerbations of fibrotic hypersensitivity pneumonitis: a case series. Chest. 2008;134(4):844–50.
Miyazaki Y, Tateishi T, Akashi T, Ohtani Y, Inase N, Yoshizawa Y. Clinical predictors and histologic appearance of acute exacerbations in chronic hypersensitivity pneumonitis. Chest. 2008;134(6):1265–70.
Tobin RW, Pope 2nd CE, Pellegrini CA, Emond MJ, Sillery J, Raghu G. Increased prevalence of gastroesophageal reflux in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 1998;158(6):1804–8.
Raghu G, Freudenberger TD, Yang S, Curtis JR, Spada C, Hayes J, et al. High prevalence of abnormal acid gastro-oesophageal reflux in idiopathic pulmonary fibrosis. Eur Respir J. 2006;27(1):136–42.
Marik PE. Aspiration pneumonitis and aspiration pneumonia. N Engl J Med. 2001;344(9):665–71.
Lee JS, Collard HR, Raghu G, Sweet MP, Hays SR, Campos GM, et al. Does chronic microaspiration cause idiopathic pulmonary fibrosis? Am J Med. 2010;123(4):304–11.
Lee JS, Song JW, Wolters PJ, Elicker BM, King Jr TE, Kim DS, et al. Bronchoalveolar lavage pepsin in acute exacerbation of idiopathic pulmonary fibrosis. Eur Respir J. 2012;39(2):352–8.
Tcherakian C, Cottin V, Brillet PY, Freynet O, Naggara N, Carton Z, et al. Progression of idiopathic pulmonary fibrosis: lessons from asymmetrical disease. Thorax. 2011;66(3):226–31.
McMillan TR, Moore BB, Weinberg JB, Vannella KM, Fields WB, Christensen PJ, et al. Exacerbation of established pulmonary fibrosis in a murine model by gammaherpesvirus. Am J Respir Crit Care Med. 2008;177(7):771–80.
Tomioka H, Sakurai T, Hashimoto K, Iwasaki H. Acute exacerbation of idiopathic pulmonary fibrosis: role of Chlamydophila pneumoniae infection. Respirology. 2007;12(5):700–6.
Huie TJ, Olson AL, Cosgrove GP, Janssen WJ, Lara AR, Lynch DA, et al. A detailed evaluation of acute respiratory decline in patients with fibrotic lung disease: aetiology and outcomes. Respirology. 2010;15(6):909–17.
Wootton SC, Kim DS, Kondoh Y, Chen E, Lee JS, Song JW, et al. Viral infection in acute exacerbation of idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;183(12):1698–702.
Mukae H, Iiboshi H, Nakazato M, Hiratsuka T, Tokojima M, Abe K, et al. Raised plasma concentrations of alpha-defensins in patients with idiopathic pulmonary fibrosis. Thorax. 2002;57(7):623–8.
Konishi K, Gibson KF, Lindell KO, Richards TJ, Zhang Y, Dhir R, et al. Gene expression profiles of acute exacerbations of idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2009;180(2):167–75.
Kurosu K, Takiguchi Y, Okada O, Yumoto N, Sakao S, Tada Y, et al. Identification of annexin 1 as a novel autoantigen in acute exacerbation of idiopathic pulmonary fibrosis. J Immunol. 2008;181(1):756–67.
Moeller A, Gilpin SE, Ask K, Cox G, Cook D, Gauldie J, et al. Circulating fibrocytes are an indicator of poor prognosis in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2009;179(7):588–94.
Ebina M, Taniguchi H, Miyasho T, Yamada S, Shibata N, Ohta H, et al. Gradual increase of high mobility group protein b1 in the lungs after the onset of acute exacerbation of idiopathic pulmonary fibrosis. Pulm Med. 2011;2011:916486.
Abe S, Hayashi H, Seo Y, Matsuda K, Kamio K, Saito Y, et al. Reduction in serum high mobility group box-1 level by polymyxin B-immobilized fiber column in patients with idiopathic pulmonary fibrosis with acute exacerbation. Blood Purif. 2011;32(4):310–6.
Collard HR, Calfee CS, Wolters PJ, Song JW, Hong SB, Brady S, et al. Plasma biomarker profiles in acute exacerbation of idiopathic pulmonary fibrosis. Am J Physiol Lung Cell Mol Physiol. 2010;299(1):L3–7.
Yokoyama A, Kohno N, Hamada H, Sakatani M, Ueda E, Kondo K, et al. Circulating KL-6 predicts the outcome of rapidly progressive idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 1998;158(5 Pt 1):1680–4.
Tajima S, Oshikawa K, Tominaga S, Sugiyama Y. The increase in serum soluble ST2 protein upon acute exacerbation of idiopathic pulmonary fibrosis. Chest. 2003;124(4):1206–14.
Ambrosini V, Cancellieri A, Chilosi M, Zompatori M, Trisolini R, Saragoni L, et al. Acute exacerbation of idiopathic pulmonary fibrosis: report of a series. Eur Respir J. 2003;22(5):821–6.
Akira M, Kozuka T, Yamamoto S, Sakatani M. Computed tomography findings in acute exacerbation of idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2008;178(4):372–8.
Parambil JG, Myers JL, Ryu JH. Histopathologic features and outcome of patients with acute exacerbation of idiopathic pulmonary fibrosis undergoing surgical lung biopsy. Chest. 2005;128(5):3310–5.
Rice AJ, Wells AU, Bouros D, du Bois RM, Hansell DM, Polychronopoulos V, et al. Terminal diffuse alveolar damage in relation to interstitial pneumonias. An autopsy study. Am J Clin Pathol. 2003;119(5):709–14.
Churg A, Muller NL, Silva CI, Wright JL. Acute exacerbation (acute lung injury of unknown cause) in UIP and other forms of fibrotic interstitial pneumonias. Am J Surg Pathol. 2007;31(2):277–84.
Akira M, Hamada H, Sakatani M, Kobayashi C, Nishioka M, Yamamoto S. CT findings during phase of accelerated deterioration in patients with idiopathic pulmonary fibrosis. AJR Am J Roentgenol. 1997;168(1):79–83.
Noble PW, Albera C, Bradford WZ, Costabel U, Glassberg MK, Kardatzke D, et al. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): two randomised trials. Lancet. 2011;377(9779):1760–9.
King Jr TE, Brown KK, Raghu G, du Bois RM, Lynch DA, Martinez F, et al. BUILD-3: a randomized, controlled trial of bosentan in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;184(1):92–9.
Fernandez Perez ER, Daniels CE, Schroeder DR, St Sauver J, Hartman TE, Bartholmai BJ, et al. Incidence, prevalence, and clinical course of idiopathic pulmonary fibrosis: a population-based study. Chest. 2010;137(1):129–37.
Kubo H, Nakayama K, Yanai M, Suzuki T, Yamaya M, Watanabe M, et al. Anticoagulant therapy for idiopathic pulmonary fibrosis. Chest. 2005;128(3):1475–82.
Azuma A, Nukiwa T, Tsuboi E, Suga M, Abe S, Nakata K, et al. Double-blind, placebo-controlled trial of pirfenidone in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2005;171(9):1040–7.
Richeldi L, Costabel U, Selman M, Kim DS, Hansell DM, Nicholson AG, et al. Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis. N Engl J Med. 2011;365(12):1079–87.
Noth I, Anstrom KJ, Calvert SB, de Andrade J, Flaherty KR, Glazer C, et al. A Placebo-controlled randomized trial of warfarin in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2012;186(1):89–95.
Raghu G, Collard HR, Egan JJ, Martinez FJ, Behr J, Brown KK, et al. An Official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011;183(6):788–824.
Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1334–49.
Weigelt JA, Norcross JF, Borman KR, Snyder 3rd WH. Early steroid therapy for respiratory failure. Arch Surg. 1985;120(5):536–40.
Peter JV, John P, Graham PL, Moran JL, George IA, Bersten A. Corticosteroids in the prevention and treatment of acute respiratory distress syndrome (ARDS) in adults: meta-analysis. BMJ. 2008;336(7651):1006–9.
Meduri GU, Golden E, Freire AX, Taylor E, Zaman M, Carson SJ, et al. Methylprednisolone infusion in early severe ARDS: results of a randomized controlled trial. Chest. 2007;131(4):954–63.
Luce JM, Montgomery AB, Marks JD, Turner J, Metz CA, Murray JF. Ineffectiveness of high-dose methylprednisolone in preventing parenchymal lung injury and improving mortality in patients with septic shock. Am Rev Respir Dis. 1988;138(1):62–8.
Bernard GR, Luce JM, Sprung CL, Rinaldo JE, Tate RM, Sibbald WJ, et al. High-dose corticosteroids in patients with the adult respiratory distress syndrome. N Engl J Med. 1987;317(25):1565–70.
Steinberg KP, Hudson LD, Goodman RB, Hough CL, Lanken PN, Hyzy R, et al. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome. N Engl J Med. 2006;354(16):1671–84.
Sakamoto S, Homma S, Miyamoto A, Kurosaki A, Fujii T, Yoshimura K. Cyclosporin A in the treatment of acute exacerbation of idiopathic pulmonary fibrosis. Intern Med. 2010;49(2):109–15.
Inase N, Sawada M, Ohtani Y, Miyake S, Isogai S, Sakashita H, et al. Cyclosporin A followed by the treatment of acute exacerbation of idiopathic pulmonary fibrosis with corticosteroid. Intern Med. 2003;42(7):565–70.
Homma S, Sakamoto S, Kawabata M, Kishi K, Tsuboi E, Motoi N, et al. Cyclosporin treatment in steroid-resistant and acutely exacerbated interstitial pneumonia. Intern Med. 2005;44(11):1144–50.
Horita N, Akahane M, Okada Y, Kobayashi Y, Arai T, Amano I, et al. Tacrolimus and steroid treatment for acute exacerbation of idiopathic pulmonary fibrosis. Intern Med. 2011;50(3):189–95.
Seo Y, Abe S, Kurahara M, Okada D, Saito Y, Usuki J, et al. Beneficial effect of polymyxin B-immobilized fiber column (PMX) hemoperfusion treatment on acute exacerbation of idiopathic pulmonary fibrosis. Intern Med. 2006;45(18):1033–8.
Miyamoto K, Tasaka S, Hasegawa N, Kamata H, Shinoda H, Kimizuka Y, et al. [Effect of direct hemoperfusion with a polymyxin B immobilized fiber column in acute exacerbation of interstitial pneumonia and serum indicators]. Nihon Kokyuki Gakkai Zasshi. 2009;47(11): 978–84.
Enomoto N, Suda T, Uto T, Kato M, Kaida Y, Ozawa Y, et al. Possible therapeutic effect of direct haemoperfusion with a polymyxin B immobilized fibre column (PMX-DHP) on pulmonary oxygenation in acute exacerbations of interstitial pneumonia. Respirology. 2008;13(3):452–60.
Nakamura M, Ogura T, Miyazawa N, Tagawa A, Kozawa S, Watanuki Y, et al. [Outcome of patients with acute exacerbation of idiopathic interstitial fibrosis (IPF) treated with sivelestat and the prognostic value of serum KL-6 and surfactant protein D]. Nihon Kokyuki Gakkai Zasshi. 2007;45(6):455–9.
Yokoyama T, Kondoh Y, Taniguchi H, Kataoka K, Kato K, Nishiyama O, et al. Noninvasive ventilation in acute exacerbation of idiopathic pulmonary fibrosis. Intern Med. 2010;49(15): 1509–14.
Gottlieb J, Warnecke G, Hadem J, Dierich M, Wiesner O, Fuhner T, et al. Outcome of critically ill lung transplant candidates on invasive respiratory support. Intensive Care Med. 2012;38(6):968–75.
Fuehner T, Kuehn C, Hadem J, Wiesner O, Gottlieb J, Tudorache I, et al. Extracorporeal membrane oxygenation in awake patients as bridge to lung transplantation. Am J Respir Crit Care Med. 2012;185(7):763–8.
Boussaud V, Mal H, Trinquart L, Thabut G, Danner-Boucher I, Dromer C, et al. One-year experience with high-emergency lung transplantation in france. Transplantation. 2012;93(10): 1058–63.
Bermudez CA, Rocha RV, Zaldonis D, Bhama JK, Crespo MM, Shigemura N, et al. Extracorporeal membrane oxygenation as a bridge to lung transplant: midterm outcomes. Ann Thorac Surg. 2011;92(4):1226–31. discussion 31-2.
Saydain G, Islam A, Afessa B, Ryu JH, Scott JP, Peters SG. Outcome of patients with idiopathic pulmonary fibrosis admitted to the intensive care unit. Am J Respir Crit Care Med. 2002;166(6):839–42.
Mollica C, Paone G, Conti V, Ceccarelli D, Schmid G, Mattia P, et al. Mechanical ventilation in patients with end-stage idiopathic pulmonary fibrosis. Respiration. 2010;79(3):209–15.
Mallick S. Outcome of patients with idiopathic pulmonary fibrosis (IPF) ventilated in intensive care unit. Respir Med. 2008;102(10):1355–9.
Blivet S, Philit F, Sab JM, Langevin B, Paret M, Guerin C, et al. Outcome of patients with idiopathic pulmonary fibrosis admitted to the ICU for respiratory failure. Chest. 2001;120(1):209–12.
Stern JB, Mal H, Groussard O, Brugiere O, Marceau A, Jebrak G, et al. Prognosis of patients with advanced idiopathic pulmonary fibrosis requiring mechanical ventilation for acute respiratory failure. Chest. 2001;120(1):213–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Lee, J.S., Collard, H.R. (2014). Acute Exacerbation of Idiopathic Pulmonary Fibrosis. In: Meyer, K., Nathan, S. (eds) Idiopathic Pulmonary Fibrosis. Respiratory Medicine, vol 9. Humana Press, Totowa, NJ. https://doi.org/10.1007/978-1-62703-682-5_17
Download citation
DOI: https://doi.org/10.1007/978-1-62703-682-5_17
Published:
Publisher Name: Humana Press, Totowa, NJ
Print ISBN: 978-1-62703-681-8
Online ISBN: 978-1-62703-682-5
eBook Packages: MedicineMedicine (R0)