
Abstract
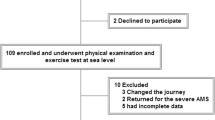
In mountaineers, recent altitude exposure has been shown to improve climbing performance and clinical outcomes during re-exposure to high altitude. However, the timing of previous altitude exposure has not been clearly reported and previous findings might be driven by individuals who were still acclimatised at the time of re-exposure. Our goal was to determine whether recent altitude exposure would confer an advantage even in individuals who had de-acclimatised for ≥1 week before being re-exposure. Low-altitude natives kept a daily trekking log throughout 7- to 8-day trek from Lukla (2,840 m) to Gokyo Ri (5,360 m). Trekkers with recent altitude exposure (re-acclimatisers, RA; n = 20) walked 20% faster (p < 0.01), reported lower acute mountain sickness scores (9 ± 8 vs. 15 ± 13; p = 0.02), and used less medication to treat headache (p < 0.05) compared to trekkers with no recent altitude exposure (initial acclimatisers, IA; n = 30). On Gokyo Ri, SpO2 was significantly higher in RA than IA trekkers (85 ± 6 vs. 78 ± 6; p = 0.01). These data indicate improved functional outcomes and physiological compensation for hypoxia in RA. However, even after de-acclimatisation for 7–30 days, it is possible that RA trekkers began the trek in a more acclimatised state than IA trekkers. RA trekkers might represent a self-selected group that has previously tolerated altitude well and has therefore opted to return. Some findings might also reflect improved psychological altitude tolerance in RA. A direct comparison of the functional and physiological responses to hypoxia throughout an initial and re-acclimatisation to high altitude is needed.
Similar content being viewed by others

References
Beidleman BA, Muza SR, Rock PB, Fulco CS, Lyons TP, Hoyt RW, Cymerman A (1997) Exercise responses after altitude acclimatization are retained during reintroduction to altitude. Med Sci Sports Exerc 29:1588–1595
Beidleman BA, Muza SR, Fulco CS, Cymerman A, Ditzler D, Stulz D, Staab JE, Skrinar GS, Lewis SF, Sawka MN (2004) Intermittent altitude exposures reduce acute mountain sickness at 4300 m. Clin Sci (Lond) 106:321–328
Benoit H, Germain M, Barthelemy JC, Denis C, Castells J, Dormois D, Lacour JR, Geyssant A (1992) Pre-acclimatization to high altitude using exercise with normobaric hypoxic gas mixtures. Int J Sports Med 13(Suppl 1):S213–S216
Bircher HP, Eichenberger U, Maggiorini M, Oelz O, Bärtsch P (1994) Relationship of mountain-sickness to physical-fitness and exercise intensity during ascent. J Wilderness Med 5:302–311
Borg GA (1982) Psychophysical bases of perceived exertion. Med Sci Sports Exerc 14:377–381
Bradshaw DI, George JD, Hyde A, LaMonte MJ, Vehrs PR, Hager RL, Yanowitz FG (2005) An accurate VO2max nonexercise regression model for 18–65-year-old adults. Res Q Exerc Sport 76:426–432
Calbet JA, Boushel R, Radegran G, Sondergaard H, Wagner PD, Saltin B (2003) Why is VO2max after altitude acclimatization still reduced despite normalization of arterial O2 content? Am J Physiol Regul Integr Comp Physiol 284:R304–R316
Cymerman A, Jaeger JJ, Kobrick JL, Maher JJ (1979) Physical fitness and acute mountain sickness (AMS). 1979 Banff Hypoxia Symposium. Arctic Insititute of North America, Calgary
Dempsey JA, Forster HV, DoPico GA (1974) Ventilatory acclimatization to moderate hypoxemia in man. The role of spinal fluid (H+). J Clin Invest 53:1091–1100
Farias JG, Osorio J, Soto G, Brito J, Siques P, Reyes JG (2006) Sustained acclimatization in Chilean mine workers subjected to chronic intermittent hypoxia. High Alt Med Biol 7:302–306
Hackett PH, Oelz O (1992) The Lake Louise consensus on the definition and quantification of altitude illness. In: Sutton JR, Coates G, Houston CS (eds) Hypoxia and Mountain Medicine. Queen City Printers, Burlington
Hackett PH, Rennie D (1983) Acute mountain sickness. Semin Resp Med 5:132–140
Hackett PH, Roach RC (2001) High-altitude illness. N Engl J Med 345:107–114
Heinicke K, Prommer N, Cajigal J, Viola T, Behn C, Schmidt W (2003) Long-term exposure to intermittent hypoxia results in increased hemoglobin mass, reduced plasma volume, and elevated erythropoietin plasma levels in man. Eur J Appl Physiol 88:535–543
Honigman B, Read M, Lezotte D, Roach RC (1995) Sea-level physical activity and acute mountain sickness at moderate altitude. West J Med 163:117–121
Houston CS (1997) Operation Everest one and two. Studies of acclimatization to simulated high altitude. Respiration 64:398–406
Hultgren HN (1997) High Altitude Medicine. Hultgren Publications, Stanford
Hupperets MD, Hopkins SR, Pronk MG, Tiemessen IJ, Garcia N, Wagner PD, Powell FL (2004) Increased hypoxic ventilatory response during 8 weeks at 3800 m altitude. Respir Physiol Neurobiol 142:145–152
Lyons TP, Muza SR, Rock PB, Cymerman A (1995) The effect of altitude pre-acclimatization on acute mountain sickness during reexposure. Aviat Space Environ Med 66:957–962
MacNutt MJ (2011) Acclimatisation, de-acclimatisation and re-acclimatisation to hypoxia. School of Human Kinetics, University of British Columbia, Vancouver, p 211
MacNutt MJ, Laursen PB, Kedia S, Neupane M, Parajuli P, Pokharel J, Sheel AW (2009) Destination Gokyo: acclimatisation and re-acclimatisation in high altitude trekkers. International Hypoxia Symposia, Lake Louise
Mani MS (1990) Fundamentals of High Altitude Biology. Oxford & IBH Publishing Co. Pvt. Ltd., New Delhi
Menon ND (1965) High-altitude pulmonary edema: a clinical study. N Engl J Med 273:66–73
Milledge JS, Ward MP, Williams ES, Clarke CR (1983) Cardiorespiratory response to exercise in men repeatedly exposed to extreme altitude. J Appl Physiol 55:1379–1385
Milledge JS, Beeley JM, Broome J, Luff N, Pelling M, Smith D (1991) Acute mountain sickness susceptibility, fitness and hypoxic ventilatory response. Eur Respir J 4:1000–1003
Mirrakhimov MM, Winslow RM (1996) The cardiovascular system at high altitude. In: Fregly MJ, Blatteis CM (eds) Environmental Physiology. Oxford University Press, New York, pp 1241–1257
Noël-Jorand MC, Reinert M, Bonnon M, Therme P (1995) Discourse analysis and psychological adaptation to high-altitude hypoxia. Stress Med 11:27–39
O’Connor T, Dubowitz G, Bickler PE (2004) Pulse oximetry in the diagnosis of acute mountain sickness. High Alt Med Biol 5:341–348
Pesce C, Leal C, Pinto H, Gonzalez G, Maggiorini M, Schneider M, Bärtsch P (2005) Determinants of acute mountain sickness and success on Mount Aconcagua (6962 m). High Alt Med Biol 6:158–166
Pugh L (1962) Physiological and medical aspects of the Himalayan scientific and mountaineering expedition, 1960–61. Br Med J 5305:621–627
Richalet JP, Bittel J, Herry JP, Savourey G, Le Trong JL, Auvert JF, Janin C (1992) Use of a hypobaric chamber for pre-acclimatization before climbing Mount Everest. Int J Sports Med 13(Suppl 1):S216–S220
Richalet JP, Robach P, Jarrot S, Schneider JC, Mason NP, Cauchy E, Herry JP, Bienvenu A, Gardette B, Gortan C (1999) Operation Everest III (Comex ‘97). Adv Exp Med Biol 474:297–317
Richalet JP, Donoso MV, Jimenez D, Antezana AM, Hudson C, Cortes G, Osorio J, Leon A (2002) Chilean miners commuting from sea level to 4500 m: a prospective study. High Alt Med Biol 3:159–166
Roach RC, Bärtsch P, Oelz O, Hackett PH (1993) The Lake Lousie acute mountain sickness scoring system. In: Sutton JR, Houston C, Coates G (eds) Hypoxia and Molecular Medicine. Queen City Press, Burlington
Rose MS, Houston CS, Fulco CS, Coates G, Sutton JR, Cymerman A (1988) Operation Everest II: nutrition and body composition. J Appl Physiol 65:2545–2551
Savourey G, Garcia N, Besnard Y, Hanniquet AM, Fine MO, Bittel J (1994) Physiological changes induced by pre-adaptation to high altitude. Eur J Appl Physiol Occup Physiol 69:221–227
Schneider M, Bernasch D, Weymann J, Holle R, Bärtsch P (2002) Acute mountain sickness: influence of susceptibility, preexposure, and ascent rate. Med Sci Sports Exerc 34:1886–1891
Schoene RB, Lahiri S, Hackett PH, Peters RM Jr, Milledge JS, Pizzo CJ, Sarnquist FH, Boyer SJ, Graber DJ, Maret KH et al (1984) Relationship of hypoxic ventilatory response to exercise performance on Mount Everest. J Appl Physiol 56:1478–1483
Seiler KS, Kjerland GO (2006) Quantifying training intensity distribution in elite endurance athletes: is there evidence for an “optimal” distribution? Scand J Med Sci Sports 16:49–56
Singh MV, Rawal SB, Tyagi AK, Bhagat JK, Parshad R, Divekar HM (1988) Changes in body fluid compartments on re-induction to high altitude and effect of diuretics. Int J Biometeorol 32:36–40
Tsianos G, Woolrich-Burt L, Aitchison T, Peacock A, Watt M, Montgomery H, Watt I, Grant S (2006) Factors affecting a climber’s ability to ascend Mont Blanc. Eur J Appl Physiol 96:32–36
Ward MP, Milledge JS, West JB (2000) Altitude acclimatization. In: Ward MP, Milledge JS, West JB (eds) High Altitude Medicine and Physiology. Oxford University Press, New York, pp 44–49
Westerterp KR, Meijer EP, Rubbens M, Robach P, Richalet JP (2000) Operation Everest III: energy and water balance. Pflugers Arch 439:483–488
Ziaee V, Yunesian M, Ahmadinejad Z, Halabchi F, Kordi R, Alizadeh R, Afsharjoo HR (2003) Acute mountain sickness in Iranian trekkers around Mount Damavand (5671 m) in Iran. Wilderness Environ Med 14:214–219
Acknowledgments
This work was supported by the Natural Sciences and Engineering Research Council of Canada. MJM received support from the Heart and Stroke Foundation of Canada. The authors would like to graciously acknowledge the assistance of Mr. Funuru Sherpa and Mr. Kami Nuru Sherpa.
Conflict of interest
None to declare.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Guido Ferretti.
Rights and permissions
About this article
Cite this article
MacNutt, M.J., Laursen, P.B., Kedia, S. et al. Acclimatisation in trekkers with and without recent exposure to high altitude. Eur J Appl Physiol 112, 3287–3294 (2012). https://doi.org/10.1007/s00421-012-2308-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-012-2308-x