
Abstract
Background
Epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) are now key agents in treating EGFR-mutant non-small cell lung cancer (NSCLC). The efficacy of gefitinib or erlotinib monotherapy can be predicted by the development of a skin rash. However, it has not been fully evaluated if this is the case with afatinib monotherapy.
Methods
We retrospectively studied 49 consecutive patients with EGFR-mutant NSCLC who received afatinib therapy between 2009 and 2015. The relationship of several toxicities with tumor response was examined.
Results
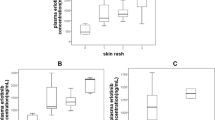
Grade 2, or more severe, common adverse events (AEs) included skin rash in 17 patients (35 %), diarrhea in 19 (39 %) and mucositis in 15 (31 %). Of these, the number of patients who developed ≥Grade 2 AEs during the first week after the initiation of afatinib therapy was: five patients had skin rash (10 %), 12 patients had diarrhea (25 %) and four patients had mucositis (8 %). As for an objective response, 21 (43 %) of the 49 had a partial response. Associating the AEs with the antitumor effect, those who had a ≥Grade 2 skin rash within the first week tended to have a greater tumor response compared with those without a rash (80 vs. 39 %; p = 0.077).
Conclusion
Our small study demonstrated that the early development of a skin rash might be associated with the response to afatinib monotherapy.
Similar content being viewed by others


References
Lynch TJ, Bell DW, Sordella R et al (2004) Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med 350:2129–2139
Paez JG, Janne PA, Lee JC et al (2004) EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science 304:1497–1500
Pao W, Miller V, Zakowski M et al (2004) EGF receptor gene mutations are common in lung cancers from “never smokers” and are associated with sensitivity of tumors to gefitinib and erlotinib. Proc Natl Acad Sci USA 101:13306–13311
Mitsudomi T, Yatabe Y (2010) Epidermal growth factor receptor in relation to tumor development: EGFR gene and cancer. FEBS J 277:301–308
Mok TS, Wu YL, Thongprasert S et al (2009) Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med 361:947–957
Maemondo M, Inoue A, Kobayashi K et al (2010) Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med 362:2380–2388
Zhou C, Wu YL, Chen G et al (2011) Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol 12:735–742
Rosell R, Carcereny E, Gervais R et al (2012) Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small cell lung cancer (EURTAC): a multicentre, open-label, randomized phase 3 trial. Lancet Oncol 13:239–246
Sequist LV, Yang JC, Yamamoto N et al (2013) Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol 31:3327–3334
Wu YL, Zhou C, Hu CP et al (2014) Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): an open-label, randomised phase 3 trial. Lancet Oncol 15:213–222
Lynch TJ, Bell DW, Sordella R et al (2004) Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med 350:2129–2139
West HL, Franklin WA, McCoy J et al (2006) Gefitinib therapy in advanced bronchioloalveolar carcinoma: Southwest Oncology Group Study S0126. J Clin Oncol 24:1807–1813
Shepherd FA, Rodrigues PJ, Ciuleanu T et al (2005) Erlotinib in previously treated non-small-cell lung cancer. N Engl J Med 353:123–132
Eisenhauer EA, Therasse P, Bogaerts J et al (2009) New response evaluation criteria in solid tumors: revised RECIST guideline (version 1.1). Eur J Cancer 45:228–247
Giaccone G, Gallegos Ruiz M, Le Chevalier T et al (2006) Erlotinib for frontline treatment of advanced non-small cell lung cancer: a phase II study. Clin Cancer Res 12:6049–6055
Cohen EE, Kane MA, List MA et al (2005) Phase II trial of gefitinib 250 mg daily in patients with recurrent and/or metastatic squamous cell carcinoma of the head and neck. Clin Cancer Res 11:8418–8424
Rudin CM, Liu W, Desai A et al (2008) Pharmacogenomic and pharmacokinetic determinants of erlotinib toxicity. J Clin Oncol 26:1119–1127
Fukudo M, Ikemi Y, Togashi Y et al (2013) Population pharmacokinetics/pharmacodynamics of erlotinib and pharmacogenomic analysis of plasma and cerebrospinal fluid drug concentrations in Japanese patients with non-small cell lung cancer. Clin Pharmacokinet 52:593–609
Wind S, Schmid M, Erhardt J et al (2013) Pharmacokinetics of afatinib, a selective irreversible ErbB family blocker, in patients with advanced solid tumours. Clin Pharmacokinet 52:1101–1109
Zhao YY, Li S, Zhang Y et al (2011) The relationship between drug exposure and clinical outcomes of non-small cell lung cancer patients treated with gefitinib. Med Oncol 28:697–702
Motoshima K, Nakamura Y, Sano K et al (2013) Phase II trial of erlotinib in patients with advanced non-small-cell lung cancer harboring epidermal growth factor receptor mutations: additive analysis of pharmacokinetics. Cancer Chemother Pharmacol 72:1299–1304
Acknowledgments
The authors acknowledge the following people for assistance and input in this trial: Kiichiro Ninomiya, Hisao Higo, Go Makimoto and Shinobu Hosokawa. The authors are also deeply grateful for all the participants who made this study possible.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
KH has received honoraria from Eli Lilly Japan, Taiho Pharmaceutical, Chugai Pharmaceutical and Sanofi-Aventis. NT has received honoraria from Eli Lilly Japan, Nihon Kayaku, AstraZeneca, Daiichi-Sankyo Pharmaceutical, Chugai Pharmaceutical, Taiho Pharmaceutical, Pfizer Inc. Japan, Boehringer-Ingelheim in Japan, and Sanofi-Aventis. NT also received research donated funds from Eli Lilly Japan, Nihon Kayaku, AstraZeneca, Chugai Pharmaceutical, Taiho Pharmaceutical, Pfizer Inc. Japan, Boehringer-Ingelheim in Japan. KK has received honoraria from Eli Lilly Japan, Nihon Kayaku, AstraZeneca, Daiichi-Sankyo Pharmaceutical, Chugai Pharmaceutical, Taiho Pharmaceutical and Sanofi-Aventis. All other authors declare that they have no conflicts of interest relating to this study.
Rights and permissions
About this article

Cite this article
Kudo, K., Hotta, K., Bessho, A. et al. Development of a skin rash within the first week and the therapeutic effect in afatinib monotherapy for EGFR-mutant non-small cell lung cancer (NSCLC): Okayama Lung Cancer Study Group experience. Cancer Chemother Pharmacol 77, 1005–1009 (2016). https://doi.org/10.1007/s00280-015-2910-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-015-2910-9