
Abstract
Purpose
Our purpose as to evaluate the impact of adjuvant radioactive iodine therapy (RAI) on prognosis, as assessed by progression-free survival (PFS) and overall survival (OS), in patients affected by differentiated thyroid carcinoma (DTC) lymph-node relapse and previously treated with lymphadenectomy.
Methods
We retrospectively evaluated DTC patients treated with lymph-node dissection for disease relapse. All patients had previously undergone total thyroidectomy and radioiodine remnant ablation (RRA). We used clinical and histological data obtained during follow-up to assess response and outcome. By means of univariate and multivariate time-to-event analyses, we assessed the impact of RAI on outcome (PFS and OS) and the prognostic role of thyroglobulin (Tg) levels under suppression with levothyroxine (Tg-on) measured 1–3 months after lymphadenectomy and of other risk factors.
Results
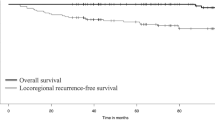
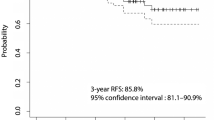
We evaluated 113 patients (age at diagnosis: median 41 years, interquartile range: 31–59), 64 of whom were treated with RAI. Over a median follow-up time of 5.7 years, 27 patients showed disease progression and 13 died. Kaplan-Meier PFS and OS curves showed that age on diagnosis, tumor histology, tumor size, DTC aggressive variant, and Tg-on were associated with prognosis. Patients with Tg-on ≥1 ng/ml treated with RAI showed a better PFS (Log-rank pp 0.001) and OS (p = 0.005) than untreated patients, while no effect of RAI was observed in patients with Tg-on <1 ng/ml. Multivariate models showed that age, Tg-on (≥1 vs. < 1 ng/ml, HR: 18.2, 95% CI: 5.09-64.8, p = 0.001) and RAI (Yes vs. No, HR: 0.36,95%CI: 0.15-0. 9, p = 0.02) remained the only independent factors associated with PFS, but only age and Tg-on remained significantly associated with OS (HR: 8.31, 95%CI:1.56-44.3, p = 0.01). Nonetheless, patients treated with RAI showed a lower risk of mortality (HR: 0.34, 95%CI: 0.1-1.15 p = 0.08) than untreated patients.
Conclusions
RAI after lymphadenectomy for DTC relapse is significantly associated with better PFS only in patients with Tg-on ≥1 ng/ml.



Similar content being viewed by others

References
Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167–214.
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26:1–133.
Pacini F, Schlumberger M, Dralle H, Elisei R, Smit JW, Wiersinga W. European Thyroid Cancer Taskforce. European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium. Eur J Endocrinol. 2006;154:787–803.
Palme CE, Waseem Z, Raza SN, Eski S, Walfish P, Freeman JL. Management and outcome of recurrent well-differentiated thyroid carcinoma. Arch Otolaryngol Head Neck Surg. 2004;130:819–24.
Tubiana M, Schlumberger M, Rougier P, Laplanche A, Benhamou E, Gardet P, et al. Long-term results and prognostic factors in patients with differentiated thyroid carcinoma. Cancer. 1985;55:794–804.
Baek SK, Jung KY, Kang SM, Kwon SY, Woo JS, Cho SH, et al. Clinical risk factors associated with cervical lymph node recurrence in papillary thyroid carcinoma. Thyroid. 2010;20:147–52.
Sugitani I, Kasai N, Fujimoto Y, Yanagisawa A. A novel classification system for patients with PTC: addition of thenewvariables of large (3 cm or greater) nodal metastases and reclassification during the follow-up period. Surgery. 2004;135:139–48.
Steward DL. Update in utility of secondary node dissection for papillary thyroid cancer. J Clin Endocrinol Metab. 2012;97(10):3393–8.
Urken ML, Milas M, Randolph GW, Tufano R, Bergman D, Bernet V, et al. Management of recurrent and persistent metastatic lymph nodes in well-differentiated thyroid cancer: amultifactorial decision-making guide for the Thyroid Cancer Care Collaborative. Head Neck. 2015;37:605–14.
Yim JH, Kim WB, Kim EY, Kim WG, Kim TY, Ryu JS, et al. Adjuvant radioactive therapy after reoperation for locoregionally recurrent papillary thyroid cancer in patients who initially underwent total thyroidectomy and high-dose remnant ablation. J Clin Endocrinol Metab. 2011;96:3695–700.
Baloch Z, LiVolsi VA, Tondon R. Aggressive variants of follicular cell derived thyroid carcinoma; the so called ‘real thyroid carcinomas’. J Clin Pathol. 2013;66:733–43.
Mazzaferri EL, Robbins RJ, Spencer CA, Braverman LE, Pacini F, Wartofsky L, et al. A consensus report of the role of serum thyroglobulin as a monitoring method for low-risk patients with papillary thyroid carcinoma. J Clin Endocrinol Metab. 2003;88:1433–41.
Piccardo A, Puntoni M, Bertagna F, Treglia G, Foppiani L, Arecco F, et al. 18F-FDG uptake as a prognostic variable in primary differentiated thyroid cancer incidentally detected by PET/CT: a multicentre study. Eur J Nucl Med Mol Imaging. 2014;41:1482–91.
Giovanella L, Trimboli P, Verburg FA, Treglia G, Piccardo A, Foppiani L, et al. Thyroglobulin levels and thyroglobulin doubling time independently predict a positive 18F-FDG PET/CT scan in patients with biochemical recurrence of differentiated thyroid carcinoma. Eur J Nucl Med Mol Imaging. 2013;40:874–80.
Kim TY, Kim WB, Kim ES, Ryu JS, Yeo JS, Kim SC, et al. Serum thyroglobulin levels atthe time of 131I remnant ablation just after thyroidectomy are useful for early prediction of clinical recurrence in low-risk patients with differentiated thyroid carcinoma. J Clin Endocrinol Metab. 2005;90:1440–5.
Piccardo A, Arecco F, Puntoni M, Foppiani L, Cabria M, Corvisieri S, et al. Focus on high-risk DTC patients: high postoperative serum thyroglobulin level is a strong predictor of disease persistence and is associated to progression-free survival and overall survival. Clin Nucl Med. 2013;38:18–24.
Polachek A, Hirsch D, Tzvetov G, Slutski I, Grozinsky-Glasberg S, Singer J, et al. Prognostic value of post-thyroidectomy thyroglobulinlevels in patients with differentiated thyroidcancer. J Endocrinol Investig. 2011;34:855–60.
Piccardo A, Arecco F, Morbelli S, Bianchi P, Barbera F, Finessi M, et al. Low thyroglobulin concentrations after thyroidectomy increase the prognostic value of undetectable thyroglobulin levels on levo-thyroxine suppressive treatment in low-risk differentiated thyroid cancer. J Endocrinol Investig. 2010;33:83–7.
Tuttle RM, Tala H, Shah J, Leboeuf R, Ghossein R, Gonen M, et al. Estimating risk of recurrence in differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnant ablation: using response to therapy variables to modify the initial risk estimates predicted by the new American Thyroid Association staging system. Thyroid. 2010;20:1341–9.
Vaisman F, Momesso D, Bulzico DA, Pessoa CH, Dias F, Corbo R, et al. Spontaneous remission in thyroid cancer patients after biochemical incomplete response to initial therapy. Clin Endocrinol. 2012;77:132–8.
Treglia G, Piccardo A, Giovanella L. 131I whole-body scan or 18F-FDG PET/CT for patients with elevated thyroglobulin and negative ultrasound? Clin Transl Imaging. 2013;1:175–83.
Pacini F, Lippi F, Formica N, Elisei R, Anelli S, Ceccarelli C, et al. Therapeutic doses of iodine-131 reveal undiagnosed metastases in thyroid cancer patients with detectable serum thyroglobulin levels. J Nucl Med. 1987;28:1888–91.
Pineda JD, Lee T, Ain K, Reynolds JC, Robbins J. Iodine- 131 therapy for thyroid cancer patients with elevated thyroglobulin and negative diagnostic scan. J Clin Endocrinol Metab. 1995;80:1488–92.
Verburg FA, Mäder U, Reiners C, Hänscheid H. Long-term survival in differentiated thyroid cancer is worse after low-activity initial post-surgical 131I therapy in both high- and low-risk patients. J Clin Endocrinol Metab. 2014;99:4487–96.
Verburg FA, Mäder U, Tanase K, Thies ED, Diessl S, Buck AK, et al. Life expectancy is reduced in differentiated thyroid cancer patients 45 years old with extensive local tumor invasion, lateral lymph node, or distant metastases at diagnosis and normal in all other DTC patients. J Clin Endocrinol Metab. 2013;98:172–80.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This research did not receive any specific grant from any funding agency in the public, commercial or non-profit sector.
Conflict of interest
The authors have nothing to disclose.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964
Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Francesco Bertagna and Luca Giovanella share senior co-authorship.
Rights and permissions
About this article

Cite this article
Piccardo, A., Puntoni, M., Bottoni, G. et al. Differentiated Thyroid Cancer lymph-node relapse. Role of adjuvant radioactive iodine therapy after lymphadenectomy. Eur J Nucl Med Mol Imaging 44, 926–934 (2017). https://doi.org/10.1007/s00259-016-3593-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-016-3593-0