
Abstract
Background
Prolonged administration of benzodiazepines and/or opioids to children in a pediatric intensive care unit (PICU) may induce physiological dependence and withdrawal symptoms.
Objective
We reviewed the literature for relevant contributions on the nature of these withdrawal symptoms and on availability of valid scoring systems to assess the extent of symptoms.
Methods
The databases PubMed, CINAHL, and Psychinfo (1980–June 2006) were searched using relevant key terms.
Results
Symptoms of benzodiazepine and opioid withdrawal can be classified in two groups: central nervous system effects and autonomic dysfunction. However, symptoms of the two types show a large overlap for benzodiazepine and opioid withdrawal. Symptoms of gastrointestinal dysfunction in the PICU population have been described for opioid withdrawal only. Six assessment tools for withdrawal symptoms are used in children. Four of these have been validated for neonates only. Two instruments are available to specifically determine withdrawal symptoms in the PICU: the Sedation Withdrawal Score (SWS) and the Opioid Benzodiazepine Withdrawal Scale (OBWS). The OBWS is the only available assessment tool with prospective validation; however, the sensitivity is low.
Conclusions
Withdrawal symptoms for benzodiazepines and opioids largely overlap. A sufficiently sensitive instrument for assessing withdrawal symptoms in PICU patients needs to be developed.
Similar content being viewed by others


Introduction
Ventilated, critically ill children commonly receive sedative and analgesic drugs to ease their mental burden, anxiety and pain, induced by frightening or painful interventions and environmental factors in the pediatric intensive care unit (PICU). Intravenous opioids (such as morphine and fentanyl) and benzodiazepines (such as midazolam) are the most commonly used drugs for this purpose [1, 2]. Tolerance and physiological dependence may develop during long-term administration of opioids and/or benzodiazepines and are risk factors contributing to withdrawal symptoms precipitated by too rapid tapering or cessation of these medications [3]. Tolerance is defined as a decrease in a drug's effect or the need to increase the dose to achieve the same effect [3, 4]. Physiological dependence is the requirement for continued administration of a sedative or analgesic to prevent signs of withdrawal [4]. Psychological dependence is the need for a substance because of its euphoric effects and is encountered in the care and treatment of drug addicts [5]. Discontinuation of medication in dependent patients leads to symptoms of withdrawal [5].
Most of our knowledge on tolerance and withdrawal symptoms has been derived from research in newborns of drug-addicted mothers [6, 7] and from the literature on adult opium-addicted patients. Benzodiazepine withdrawal is also reported in adult psychiatric and drug-addicted populations [8–10]. Two retrospective and one prospective randomized controlled trial have been reported on opioid and/or benzodiazepine withdrawal after long-term administration of analgesics or sedatives in the adult ICU setting [11–13]. The reported incidence of withdrawal syndrome in adult ICU patients ranges from 32.1% (9/28) to 100% [11, 12]. Each of these studies used a different assessment tool, however, which makes it difficult to describe symptoms in a uniform manner. Symptoms in these patients are mostly agitation, irritability, anxiety, insomnia, tachycardia, hypertension, and sweating. High total doses and exposure to medication for longer than 7 days are risk factors for developing withdrawal symptoms in the adult ICU. This knowledge may serve to gain a better insight into problems of tolerance, dependence, and withdrawal in pediatric intensive care, which are still insufficiently recognized [14]. Recognition of withdrawal in PICU patients is difficult because the symptoms may strongly overlap clinical signs of inadequate sedation, such as agitation, anxiety, and movement disorder. An objective instrument to establish withdrawal symptoms of critically ill children in clinical practice is necessary to establish severity and course of the symptoms and to evaluate efficacy of withdrawal treatment.
This review of the literature addresses two questions. First, what withdrawal symptoms resulting from long-term use of sedatives (opioids and/or benzodiazepines) in critically ill children in a PICU have been described and might be useful in an assessment tool? Second, are there any validated, reliable tools to assess withdrawal symptoms in children in a PICU in clinical practice?
Methods
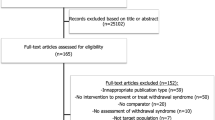
The databases PubMed, CINAHL, and Psychinfo were searched for relevant literature on (a) benzodiazepine and opioid withdrawal symptoms or (b) assessment tools for withdrawal symptoms. Time limits were set at January 1980 and May 2006. Only articles published in English or Dutch were included in the study. The following exploded MeSH terms were used: “withdrawal symptoms”, “abstinence syndrome”, “tolerance” with “opioid”, “benzodiazepine”, and with “PICU”, “critically ill children”, or with “assessment tool”, “scoring system”. The age limits were set at 0 and 16 years. Preterm neonates (< 37 weeks gestation) and neonates of addicted mothers were excluded because generally they are not admitted to a PICU. A first search for reviews retrieved seven relevant articles which were used to delineate the domain of withdrawal symptoms [3–5, 7, 15–17]. Two of these reviews relate to patients in a neonatal ICU [7, 15]. They were nevertheless included because PICUs admit surgical neonates as well. Also, these two reviews did not focus on neonates of addicted mothers.
In total, abstracts of 53 articles were evaluated. Articles on withdrawal symptoms had to meet two criteria for inclusion in this review: describing a study of benzodiazepine and/or opioid withdrawal symptoms and relating to the age restriction. In total 20 articles, either case studies, retrospective or prospective studies, met these criteria [18–37]. Table 1 lists the studies from which the withdrawal symptoms were derived, grouped by type of medication, study design, and methodological quality. Studies on assessment tools for identifying withdrawal symptoms had to meet the following criteria: (a) the tool should be aimed at identifying symptoms of benzodiazepine and/or opioid withdrawal; (b) the tool should be appropriate for children. Two articles met these criteria [17, 29].
Results
Withdrawal symptoms
Opioid withdrawal symptoms
Clinical signs of opioid withdrawal in newborns include those of the neurological system (high-pitched crying, irritability, increased wakefulness, hyperactive deep tendon reflexes, increased muscle tone, tremors, exaggerated Moro-reflex, seizures, intraventricular hemorrhage), those of the gastrointestinal tract (poor feeding, uncoordinated and/or constant sucking, vomiting, diarrhea, dehydration), autonomic signs (increased sweating, nasal stuffiness, fever, mottling), and others (poor weight gain, increased rapid-eye movement sleep, skin excoriation) [6, 15]. Symptoms of opioid withdrawal in newborns of drug-addicted mothers are generally divided into three main groups: overstimulation of the central nervous system (CNS), gastrointestinal dysfunction, and autonomic dysregulation or sympathetic hyperactivity [4, 15, 38]. Table 2 lists the described signs and symptoms of withdrawal in children relating to either opioids or benzodiazepines, or combined use, broken down for these three groups. (a) Common manifestations of CNS overstimulation are: tremors, increased muscle tension, anxiety, restlessness, irritability, and insomnia [21, 23–27, 29, 30, 32, 33]. In addition, Lane et al. [26] and French and Nocera [30] described the development of choreoathetoid movements as a withdrawal symptom of fentanyl administration in five children and one child, respectively, as well as intermittent muscle contractions and uncontrolled movements after long-term use of fentanyl. (b) The most frequent gastrointestinal symptoms of opioid withdrawal are vomiting and diarrhea [23–25, 27, 29, 32]. Carnevale and Ducharme [32] in addition reported reduced oral intake. (c) Autonomic phenomena are: fever, perspiration, sneezing, yawning, increased heart rate, and blood pressure [23–25, 29, 30]. Note that increases in heart rate and blood pressure should be seen in relation to the normal values for the child's age and disease. In summary, the clinical signs of opioid withdrawal in children (Table 2) are largely congruent with those in newborn babies of drug-addicted mothers.
Benzodiazepine withdrawal symptoms
Classical characteristics of benzodiazepine withdrawal described for the domains of adult psychiatry and drug addicts care are: severe anxiety, involuntary muscle tremors, confusion, insomnia, perception disorders, depression, and generalized convulsions [4, 9]. In contrast to opioids, a systematic classification of benzodiazepine withdrawal symptoms is not available in the literature. For the sake of uniformity, however, the grouping for opioid withdrawal symptoms will be used here as well. Table 2 lists the observed withdrawal symptoms for benzodiazepines. Strikingly, most symptoms have been described on the basis of single case-reports and case series with small numbers of patients. Only two articles describe larger patient groups of 40 and 53 patients, respectively [28, 31]. Symptoms observed in these two studies were different, however, and the used observation forms included no more than five and seven symptoms, respectively. These qualitative and quantitative limitations, notably in the case studies, provide only limited insight into the symptoms of benzodiazepine withdrawal. The benzodiazepines studies were all of a descriptive nature, in contrast to the opioids studies. (a) Regarding CNS overstimulation, Sury et al. [22] in a case-report first described withdrawal symptoms resulting from long-term use of midazolam in children. Three children aged 4, 11, and 12 years received midazolam as a sedative for 7, 14 and 17 days, respectively. Within 24 h after discontinuation they showed signs of (visual) hallucinations, irritability, confusion, restlessness/agitated behavior and generalized convulsions. These are all manifestations of CNS overstimulation. Other studies report tremors, anxiety, agitation, restlessness, inconsolable crying, muscle twitching, and myoclonic movements of the extremities [18, 19, 21, 28, 29, 31–33]. (b) Regarding sympathetic hyperactivity, a case study of two children observed tachycardia and fever as benzodiazepine withdrawal reactions [19]. Others observed perspiration, insomnia and severe coughing [29, 31]. (c) Regarding gastrointestinal dysfunction, one case study of a 14-day-old newborn reported vomiting caused by a distended stomach resulting from swallowing air [19]. This single case report provides insufficient evidence to include this symptom as a benzodiazepine withdrawal symptom. Dysfunction of the gastrointestinal tract as a symptom of benzodiazepine withdrawal has not been described in adults [9, 12]. In summary, the major symptoms of benzodiazepine withdrawal in children are anxiety, tremors, and other involuntary muscle movements, irritability, perspiration and insomnia. These correspond to the classical manifestations of benzodiazepine withdrawal in adults [4, 9].
Combined benzodiazepine-opioid withdrawal symptoms
Differences between opioid and benzodiazepine withdrawal symptoms are marginal [4]. Symptoms associated with CNS overstimulation and sympathetic hyperactivity largely overlap after long-term use of benzodiazepines or opioids in children (see Table 2). However, benzodiazepine withdrawal is not associated with symptoms of the gastrointestinal tract [4, 12]. The Moro-reflex is used as an opioid withdrawal symptom in neonates [6, 15]. The Moro-reflex disappears between the ages of 1 and 3 months and is therefore never observed in children older than 3 months. The study by Franck et al. [29] included 1.5- to 28 month-old children, and the Moro-reflex was one of the items in their assessment tool. In view of the age limitation we feel it is not feasible to use this symptom as a withdrawal symptom for PICU patients [3]. Several studies found it hard to determine whether the withdrawal symptoms were specifically caused by benzodiazepines dependence because in these studies opioids (morphine, fentanyl) were administered for sedation as well [18, 21, 28, 29, 33]. This illustrates the practical limitation for describing specific benzodiazepine-related withdrawal symptoms in the PICU. From clinical experience we know that benzodiazepines and opioids are usually administered in combination for sedation and analgesia, from several days to weeks as reflected in the literature [1, 38]. Given the overlap in symptoms, it is hard to ascribe withdrawal symptoms to either opioids or benzodiazepines [21, 29, 32].
Incidences and influencing factors of benzodiazepine and opioid withdrawal
Knowledge on the incidences of benzodiazepine andopioid withdrawal symptoms in general as well as the frequencies of the separate phenomena provide clues for the symptoms to be used in an assessment tool. Furthermore, knowledge of possible risk factors for the development of withdrawal symptoms enables physicians and nurses to identify patients at risk. Only five articles describe incidences and influencing factors for the development of withdrawal symptoms after long-term use of benzodiazepines or opioids in children [27, 28, 31].
Incidence
Fonsmark et al. [31] in a retrospective study found that 14 of 40 (35%) of sedated children (6 months–14 years) developed withdrawal symptoms. A prospective study of abrupt discontinuation of midazolam in critically ill children (0–11 years) reports adverse side effects in 17% of the 53 patients [28]. Opioid withdrawal symptoms were seen in 13/23 (57%) children aged 0–22 months after prolonged continuous fentanyl administration [27]. Methods differed between these three studies. Katz et al. [27] used the Neonatal Abstinence Score (NAS) developed by Finnegan et al. [6] which has only been validated for use in newborns. Hughes et al. [28] and Fonsmark et al. [31] did not use existing tools but recorded withdrawal symptoms through self-developed observation lists. These lists included a limited number (five) of behavioral items [28, 31]. Fonsmark et al. [31] included “sweating” as a physiological item. The authors did not provide data on reliability and validity of their observation lists [28, 31]. Patients who required extracorporeal membrane oxygenation (ECMO) therapy comprised a specific PICU population. In these populations opioid withdrawal (NAS > 8) was seen in 9–57% of children [35, 37].
Influencing factors
Various authors have shown that dosing and duration of benzodiazepines or opioids influence development of withdrawal symptoms [27, 30, 31]. Fonsmark et al. [31] found a total midazolam dose higher than 60 mg/kg to be associated with the occurrence of withdrawal symptoms. Katz et al. [27] found a total fentanyl dose of 2.5 mg/kg or higher or a fentanyl infusion for at least 9 days to result in withdrawal symptoms in 100% of cases. Arnold et al. [35] found that neonates receiving ECMO therapy with total doses greater than 1.6 mg/kg fentanyl or an ECMO duration of longer than 5 days had a significantly greater incidence of withdrawal symptoms reflected by the NAS. In another study in ECMO patients the authors demonstrated that neonates who received total fentanyl doses higher than 1.2 mg/kg were 13 times more likely to experience opioid withdrawal after ECMO [37]. Evaluation of the various studies reveals that children in a PICU receiving benzodiazepines and/or opioids for 5 days or longer are at risk for developing withdrawal symptoms [17, 23–25, 27–31]. Benzodiazepine and/or opioid withdrawal symptoms may occur if these medications are abruptly stopped or tapered off too rapidly in children showing physical dependence [38]. Manifestations typically occur 8–48 h after discontinuation.
Systematic clinical assessment of withdrawal symptoms
The task of assessing seriously ill children for signs of tolerance, dependence, or withdrawal notably falls to the pediatric critical care nurse [4]. This requires particularly awareness, knowledge of and insight into these phenomena. For clinical purposes a validated and reliable assessment tool would be very helpful. Table 3 provides details of six assessment tools for withdrawal symptoms in children that are used in practice and in research. Four of these were developed and validated for application in neonates after long-term use of opioids or in newborn babies of drug-addicted mothers [6, 39–41]. The most widely used is the NAS [6]. These four instruments have not been validated for use in older children. However, in the absence of a validated and reliable instrument for children, several authors have opted for the NAS [24, 25, 27, 30]. Other authors designed observation checklists themselves, including 5–13 symptoms [25, 38, 31]. These observation checklists have not been properly validated for use in children [25, 31]. Two recent articles describe assessment tools for observing withdrawal symptoms after long-term use of opioids and/or benzodiazepines in children in a PICU: the Sedation Withdrawal Score (SWS) [17] and the Opioid Benzodiazepine Withdrawal Scale (OBWS) [29].
Sedation Withdrawal Score
The SWS includes 12 symptoms of withdrawal (see Table 3) and was developed in 2004 by Cunliffe et al. [17]. Each symptom is scored on a three-point scale, ranging from absent (0), mild (1), to severe (2). Thus a maximum score of 24 is possible. The authors provide instructions for the regimen for decreasing sedatives based on cutoff points. However, a justification for these cutoff points is not given. The authors consider the SWS to be clinically sensitive in detecting abstinence in a child of any age with signs of withdrawal from sedatives and/or opioids [17]. However, data on sensitivity, specificity, validity, and reliability are lacking.
Opioid and Benzodiazepine Withdrawal Scale
The OBWS is a 21-item checklist with 16 withdrawal items for determining frequency and severity of withdrawal symptoms in children (see Table 3) [29]. Franck et al. [29] tested the predictive validity of the OBWS by performing 693 assessments in 15 children aged 6 weeks–28 months. Sensitivity of the OBWS at scores 8 (cutoff) or higher was 50%, which implies that the scale is not better than chance prediction. Specificity was 87%, which implies that the scale rightly classifies 87% of the children without withdrawal symptoms. The predictive value expressed in terms of positive and negative likelihood ratio, 4.0 and 0.57, respectively, is moderate for a diagnostic instrument. The interrater reliability was higher than 0.8; the agreement procedure, however, was not published. Neither age range nor diagnoses of the patients in this study are representative for a general PICU. Finally, including the Moro-reflex is questionable in view of the inherent age restriction, and reduces the scale's content validity. In summary, although both instruments include relevant withdrawal symptoms associated with benzodiazepine and/or opioid withdrawal in children, we feel that psychometric issues of the measurements have been given insufficient attention.
Discussion and conclusion
Nurses and physicians could give more priority to the observation and treatment of withdrawal symptoms in children in a PICU. This literature study describes observable withdrawal symptoms related to benzodiazepines and opioids use in children in a PICU. It appears that vomiting cannot be included as a symptom of benzodiazepine withdrawal in this population [4]. The same is true for the hyperactive Moro-reflex as a symptom of opioid withdrawal, given the age limitation [27]. Furthermore, withdrawal symptoms for benzodiazepines and opioids had a large overlap for symptoms such as agitation, anxiety, tremors, insomnia, fever, sweating, and tachycardia. Symptoms such as seizure and hallucinations have been described only as benzodiazepine withdrawal in PICU patients.
As clinical practice tends to combine medication from both groups, symptoms cannot easily be ascribed to either group. Several authors studied only either benzodiazepine or opioid withdrawal symptoms in patients who received both medications [25, 27, 28, 31]. Then it was not possible to determine whether the withdrawal symptoms were specifically caused by benzodiazepine or opioids because in these studies additional benzodiazepine or opioids were administered for sedation as well. For treatment and management purposes we should preferably distinguish between withdrawal symptoms caused by weaning of benzodiazepines or opioids. Therefore assessment tools should be sensitive enough to discriminate between benzodiazepine and opioid related withdrawal symptoms [3, 24, 42]. Generalization of the identified withdrawal symptoms is hampered by the fact that most are based on case series and case reports and consequently on small numbers of patients. Furthermore, most studies considered only few withdrawal symptoms. Thus representative incidence numbers based on the full spectrum of withdrawal symptoms are lacking.
In this review high total doses, duration of opioid, and/or benzodiazepine infusion and ECMO therapy are described as risk factors in developing withdrawal symptoms in PICU patients. These factors are also described in adult studies [11, 12]. The diagnosis of withdrawal in patients must be made carefully. Withdrawal symptoms vary from patient to patient in number, severity and presentation. However many PICU patients show relatively subtle clinical symptoms that can easily be confused with responses to other factors in the PICU. Symptoms such as agitation, anxiety, insomnia, irritability, fever, tachycardia, hypertension, and sweating are also an expression of inadequate sedation or pain management, ventilator distress, infection, noisy environment, paradoxical reactions, or delirium [43–47]. These key confounders may mask withdrawal symptoms. With Tobias [3], we maintain that the diagnosis of withdrawal symptoms remains one of exclusion. For example, fever or vomiting should never be attributed to withdrawal until other possible causes are excluded. Key confounders must be excluded as well. We feel that the occurrence of withdrawal symptoms must be time-related to a decrease or cessation of benzodiazepines and/or opioids.
Strategies to reduce the incidence of withdrawal symptoms begin by making efforts to reduce the total doses of benzodiazepines and/or opioids administered. Based on a few prospective studies several authors recommend a daily tapering rate of 10–20% for children who receive benzodiazepines and/or opioids for more than 5–7 days [23–25, 29]. This strategy did not result, however, in the absence of withdrawal symptoms. Adult sedative and analgesic guidelines recommend that daily dose decrements of opioids should not exceed 5–10% in high-risk patients [48]. Playfor et al. [49] support use of this practice in the PICU in spite of the fact that there is little evidence for its efficacy. Several studies evaluating withdrawal symptoms, incidence and risk factors in the PICU used an assessment tool (NAS) not validated for use in children in a PICU. The results of these studies therefore may not be reliable, and symptoms may have been overlooked. Most of these scoring systems (four of six, see Table 3) were developed to assess the severity of withdrawal in infants and drugs-addicted mothers. They have some limitations, however. First, they were developed to assess neonatal behavior and opioid withdrawal [3, 49]. Certain reflexes such as the Moro can only be judged in children below 3 months, and this implies that they cannot be used in the total PICU age group. Second, cutoff points for other patients than newborns of addicted mothers are not defined. For these reasons the NAS is less useful in PICU patients because most receive both opioids and benzodiazepines.
The available literature demonstrates that a good assessment tool for clinical use in children is lacking [49]. A good assessment tool can be defined as a tool, which is valid reliable, and clinically useful. This means that a cutoff point is established, and that the tool shows sensitivity to change [50, 51]. Furthermore Franck et al. [29] stated that clinical utility may be improved with fewer items and longer intervals between assessments. The OBWS displays moderate validity and includes an item that is not representative for the target population. We agree with Cunliffe et al. [17] that the SWS includes clinically relevant items for the observation of withdrawal symptoms in children on the basis of the described withdrawal symptoms in our literature study. However, it lacks a good methodological foundation. The OBWS is the only available assessment tool with prospective validation; however, its sensitivity is low. In general, assessment tools must preferably be tested in a multicenter study with a larger patient population and an extensive patient mix. The criterion validity can be tested using an independent expert's opinion because there is no gold standard for opioid and benzodiazepine withdrawal in children. Further assessments should be carried out before and after tapering off of opioids or benzodiazepines. At least key confounders that mask withdrawal must be excluded. In conclusion, the OBWS can be feasible for assessing benzodiazepine and/or opioid withdrawal symptoms in children in a PICU when additional validation has been completed.
This review clearly provides directions for further research. First, quantification of withdrawal symptoms in children based on the symptoms and signs listed in this review is needed to clearly define the spectrum of withdrawal in PICU patients. Second, an adapted withdrawal assessment tool based on this quantification needs to be developed and psychometric issues must be tested before application in the PICU population.
References
Polaner DM (2001) Sedation-analgesia in the pediatric intensive care unit. Pediatr Clin North Am 48:695–714
Jenkins I (2002) The provision of analgesia and sedation in the PICU: current practice and recent advances. Paediatr Anaesth 12:837–839
Tobias JD (2000) Tolerance, withdrawal, and physical dependency after long-term sedation and analgesia of children in the pediatric intensive care unit. Crit Care Med 28:2122–2132
Anand KJ, Ingraham J (1996) Pediatric. Tolerance, dependence, and strategies for compassionate withdrawal of analgesics and anxiolytics in the pediatric ICU. Crit Care Nurs 16:87–93
Anand KJ, Arnold JH (1994) Opioid tolerance and dependence in infants and children. Crit Care Med 22:334–342
Finnegan LP, Kron RE, Connaughton JF, Emich JP (1975) Assessment and treatment of abstinence in the infant of the drug-dependent mother. Int J Clin Pharmacol Biopharm 12:19–32
Suresh S, Anand KJ (2001) Opioid tolerance in neonates: a state-of-the-art review. Paediatr Anaesth 11:511–521
Levy AB (1984) Delirium and seizures due to abrupt alprazolam withdrawal: case report. J Clin Psychiatry 45:38–39
MacKinnon GL, Parker WA (1982) Benzodiazepine withdrawal syndrome: a literature review and evaluation. Am J Drug Alcohol Abuse 9:19–33
Mellman TA, Uhde TW (1986) Withdrawal syndrome with gradual tapering of alprazolam. Am J Psychiatry 143:1464–1466
Brown C, Albrecht R, Pettit H, McFadden T, Schermer C (2000) Opioid and benzodiazepine withdrawal syndrome in adult burn patients. Am Surg 66:367–370
Cammarano WB, Pittet JF, Weitz S, Schlobohm RM, Marks JD (1998) Acute withdrawal syndrome related to the administration of analgesic and sedative medications in adult intensive care unit patients. Crit Care Med 26:676–684
Korak-Leiter M, Likar R, Oher M, Trampitsch E, Ziervogel G, Levy JV, Freye EC (2005) Withdrawal following sufentanil/propofol and sufentanil/midazolam. Intensive Care Med 31:380–387
Marx CM, Rosenberg DI, Ambuel B, Hamlett KW, Blumer JL (1993) Pediatric intensive care sedation: survey of fellowship training programs. Pediatrics 91:369–378
Suresh S, Anand KJ (1998) Opioid tolerance in neonates: mechanisms, diagnosis, assessment, and management. Semin Perinatol 22:425–433
Puntillo K, Casella V, Reid M (1997) Opioid and benzodiazepine tolerance and dependence: application of theory to critical care practice. Heart Lung 26:317–324
Cunliffe M, McArthur L, Dooley F (2004) Managing sedation withdrawal in children who undergo prolonged PICU admission after discharge to the ward. Paediatr Anaesth 14:293–298
Yaster M, Kost-Byerly S, Berde C, Billet C (1996) The management of opioid and benzodiazepine dependence in infants, children, and adolescents. Pediatrics 98:135–140
Engelen BG van, Gimbrere JS, Booy LH (1993) Benzodiazepine withdrawal reaction in two children following discontinuation of sedation with midazolam. Ann Pharmacother 27:579–581
Tobias JD (1999) Subcutaneous administration of fentanyl and midazolam to prevent withdrawal after prolonged sedation in children. Crit Care Med 27:2262–2265
Tobias JD, Deshpande JK, Gregory DF (1994) Outpatient therapy of iatrogenic drug dependency following prolonged sedation in the pediatric intensive care unit. Intensive Care Med 20:504–507
Sury MR, Billingham I, Russell GN, Hopkins CS, Thornington R, Vivori E (1989) Acute benzodiazepine withdrawal syndrome after midazolam infusions in children. Crit Care Med 17:301–302
Siddappa R, Fletcher JE, Heard AMB, Kielma D, Cimino M, Heard CMB (2003) Methadone dosage for prevention of opioid withdrawal in children. Pediatric Anesthesia 13:805–810
Robertson RC, Darsey E, Fortenberry JD, Pettignano R, Hartley G (2000) Evaluation of an opiate-weaning protocol using methadone in pediatric intensive care unit patients. Pediatr Crit Care Med 1:119–123
Lugo RA, MacLaren R, Cash J, Pribble CG, Vernon DD (2001) Enteral methadone to expedite fentanyl discontinuation and prevent opioid abstinence syndrome in the PICU. Pharmacotherapy 21:1566–1573
Lane JC, Tennison MB, Lawless ST, Greenwood RS, Zaritisky AL (1991) Movement disorder after withdrawal of fentanyl infusion. J Pediatr 119:649–651
Katz R, Kelly HW, Hsi A (1994) Prospective study on the occurrence of withdrawal in critically ill children who receive fentanyl by continuous infusion. Crit Care Med 22:763–767
Hughes J, Gill A, Leach HJ, Nunn AJ, Billingham I, Ratcliffe J, Thornington R, Choonara I (1994) A prospective study of the adverse effects of midazolam on withdrawal in critically ill children. Acta Paediatr 83:1194–1199
Franck LS, Naughton I, Winter I (2004) Opioid and benzodiazepine withdrawal symptoms in paediatric intensive care patients. Intensive Crit Care Nurs 20:344–351
French JP, Nocera M (1994) Drug withdrawal symptoms in children after continuous infusions of fentanyl. J Pediatr Nurs 9:107–113
Fonsmark L, Rasmussen YH, Carl P (1999) Occurrence of withdrawal in critically ill sedated children. Crit Care Med 27:196–199
Carnevale FA, Ducharme C (1997) Adverse reactions to the withdrawal of opioids and benzodiazepines in paediatric intensive care. Intensive Crit Care Nurs 13:181–188
Bergman I, Steeves M, Burckart G, Thompson A (1991) Reversible neurologic abnormalities associated with prolonged intravenous midazolam and fentanyl administration. J Pediatr 119:644–649
Ducharme C, Carnevale FA, Clermont MS, Shea S (2005) A prospective study of adverse reactions to the weaning of opioids and benzodiazepines among critically ill children. Intensive Crit Care Nurs 21:179–186
Arnold JH, Truog RD, Orav EJ, Scavone JM, Hershenson MB (1990) Tolerance and dependence in neonates sedated with fentanyl during extracorporeal membrane oxygenation. Anesthesiology 73:1136–1140
Berens RJ, Meyer MT, Mikhailov TA, Colpaert KD, Czarnecki ML, Ghanayem NS, Hoffman GM, Soetenga DJ, Nelson TJ, Weisman SJ (2006) A prospective evaluation of opioid weaning in opioid-dependent pediatric critical care patients. Anesth Analg 102:1045–1050
Franck LS, Vilardi J, Durand D, Powers R (1998) Opioid withdrawal in neonates after continuous infusions of morphine or fentanyl during extracorporeal membrane oxygenation. Am J Crit Care 7:364–369
Tobias JD (1999) Sedation and analgesia in paediatric intensive care units: a guide to drug selection and use. Paediatr Drugs 1:109–126
Green M, Suffet F (1981) The Neonatal Narcotic Withdrawal Index: a device for the improvement of care in the abstinence syndrome. Am J Drug Alcohol Abuse 8:203–213
Lipsitz PJ (1975) A proposed narcotic withdrawal score for use with newborn infants. A pragmatic evaluation of its efficacy. Clin Pediatr (Phila) 14:592–594
Zahorodny W, Rom C, Whitney W, Giddens S, Samuel M, Maichuk G, Marshall R (1998) The neonatal withdrawal inventory: a simplified score of newborn withdrawal. J Dev Behav Pediatr 19:89–93
Shafer A (1998) Complications of sedation with midazolam in the intensive care unit and a comparison with other sedative regimens. Crit Care Med 26:947–956
Golparvar M, Saghaei M, Sajedi P, Razavi SS (2004) Paradoxical reaction following intravenous midazolam premedication in pediatric patients—a randomized placebo controlled trial of ketamine for rapid tranquilization. Paediatr Anaesth 14:924–930
Lonnqvist PA, Habre W (2005) Midazolam as premedication: is the emperor naked or just half-dressed? Paediatr Anaesth 15:263–265
Menon G, Anand KJ, McIntosh N (1998) Practical approach to analgesia and sedation in the neonatal intensive care unit. Semin Perinatol 22:417–424
Playfor S, Thomas D, Choonara I (2000) Recollection of children following intensive care. Arch Dis Child 83:445–448
Schieveld JN, Leentjens AF (2005) Delirium in severely ill young children in the pediatric intensive care unit (PICU). J Am Acad Child Adolesc Psychiatry 44:392–394
Jacobi J, Fraser GL, Coursin DB, Riker RR, Fontaine D, Wittbrodt ET, Chalfin DB, Masica MF, Bjerke HS, Coplin WM, Crippen DW, Fuchs BD, Kelleher RM, Marik PE, Nasraway SA Jr, Murray MJ, Peruzzi WT, Lumb PD (2002) Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med 30:119–141
Playfor S, Jenkins I, Boyles C, Choonara I, Davies G, Haywood T, Hinson G, Mayer A, Morton N, Ralph T, Wolf A (2006) Consensus guidelines on sedation and analgesia in critically ill children. Intensive Care Med 32:1125–1136
Johnston CC (1998) Psychometric issues in the measurement of pain. In: Finley GA, McGrath PJ (eds) Measurement of pain in infants and children. IASP, Seattle, pp 5–20
Streiner DL, Norman GR (2003) Health measurement scales. A practical guide to their development and use, 3rd ed. Oxford University Press, Oxford
Acknowledgements
We thank Ko Hagoort for editing the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ista, E., van Dijk, M., Gamel, C. et al. Withdrawal symptoms in children after long-term administration of sedatives and/or analgesics: a literature review. “Assessment remains troublesome”. Intensive Care Med 33, 1396–1406 (2007). https://doi.org/10.1007/s00134-007-0696-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-007-0696-x