
Abstract
Background and Objective
Pradigastat, a novel diacylglycerol acyltransferase 1 inhibitor, is under development to treat familial chylomicronemia syndrome. The potential impact of hepatic impairment on the pharmacokinetics of pradigastat was evaluated in this study.
Methods
In this study, a single oral dose of 20 mg pradigastat was administered first to patients with mild and moderate hepatic impairment (n = 10/group) and subsequently to patients with severe hepatic impairment (n = 6). The pharmacokinetics of pradigastat were compared between each patient group and the respective matched healthy subjects.
Results
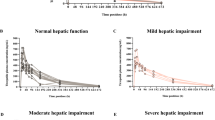
As compared with the respective matched healthy groups, the geometric mean ratios of the area under the plasma concentration–time curve from time zero to infinity (AUCinf) (h·ng/mL) were 1.49, 1.06 and 1.99 in mild, moderate and severe hepatic impairment patients, respectively; the observed maximum plasma concentration (C max) (ng/mL) values were 0.97, 1.28 and 2.74, respectively; and the total body clearance of the drug from plasma (CL/F) (L/h) values were 0.67, 0.95 and 0.50, respectively. The elimination half-life and plasma protein binding of pradigastat were comparable among all the patients. There were no apparent relationships between AUCinf or C max and albumin or bilirubin levels (R 2 < 0.3; p > 0.05). Overall, 19 adverse events (AEs) were reported in 13 patients. The incidence of AEs appeared to increase with increasing severity of hepatic impairment.
Conclusion
No clinically significant differences in the pharmacokinetics of pradigastat were observed in mild and moderate hepatic impairment patients compared with healthy subjects. However, the systemic exposure of pradigastat doubled while the clearance decreased by half in patients with severe hepatic impairment compared with healthy subjects. All treatments were well tolerated in the study.



Similar content being viewed by others


References
Meyers CD, Gaudet D, Tremblay C, et al. The DGAT1 inhibitor LCQ908 decreases triglyceride levels in patients with familial chylomicronemia syndrome. J Clin Lipidol. 2012;6:266–7.
Meyers CD, Serrano-Wu M, Amer A, et al. The DGAT1 inhibitor pradigastat decreases chylomicron secretion and prevents postprandial triglyceride elevation in humans. J Clin Lipidol. 2013;7:285.
Sugandhan S, Khandpur S, Sharma VK. Familial chylomicronemia syndrome. Pediatr Dermatol. 2007;24:323–5.
Yen CL, Stone SJ, Koliwad S, et al. Thematic review series: glycerolipids. DGAT enzymes and triacylglycerol biosynthesis. J Lipid Res. 2008;49:2283–301.
Smith SJ, Cases S, Jensen DR, et al. Obesity resistance and multiple mechanisms of triglyceride synthesis in mice lacking DGAT. Nat Genet. 2000;25:87–90.
Kulmatycki K, et al. Pharmacokinetic evaluation of escalating single intravenous and multiple oral doses of pradigastat and its absolute bioavailability in healthy subjects. Presented to the American Association of Pharmaceutical Scientists. 2013. http://abstracts.aaps.org/Verify/aaps2013/postersubmissions/R6322.pdf. Accessed 4 Sep 2014.
Yan JH, Meyers D, Lee Z, et al. Pharmacokinetic and pharmacodynamic drug–drug interaction assessment between pradigastat and digoxin or warfarin. J Clin Pharmacol. 2014;54:800–8.
Upthagrove A, et al. Disposition of pradigastat (LCQ908) in humans: in vivo and in vitro investigations. Presented at 10th International ISSX Meeting; Toronto; 2013.
Verbeeck RK. Pharmacokinetics and dosage adjustment in patients with hepatic dysfunction. Eur J Clin Pharmacol. 2008;64:1147–61.
Elbekai RH, Korashy HM, El-Kadi AO. The effect of liver cirrhosis on the regulation and expression of drug metabolizing enzymes. Curr Drug Metab. 2004;5:157–67.
Le Couteur DG, Fraser R, Hilmer S, et al. The hepatic sinusoid in aging and cirrhosis: effects on hepatic substrate disposition and drug clearance. Clin Pharmacokinet. 2005;44:187–200.
FDA guidance. Pharmacokinetics in patients with impaired hepatic function: study design, data analysis, and impact on dosing and labeling. Clin Pharmacol. 2003. http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm072123.pdf. Accessed 4 Sep 2014.
FDA draft guidance. Bioanalytical method validation. 2013 http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM368107.pdf. Accessed 10 Sep 2014.
Committee for medicinal products for human use. Guideline on the investigation of bioequivalence. 2010. http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2010/01/WC500070039.pdf. Accessed 4 Sep 2014.
Hoyumpa AM, Schenker S. Is glucuronidation truly preserved in patients with liver disease? Hepatology. 1991;13:786–95.
Sulsa GM, et al. Principles of clinical pharmacology, 2nd edn. 2007. pp. 73–87. http://carlasabandar.files.wordpress.com/2012/10/principles-of-clinical-pharmacology.pdf. Accessed 4 Sep 2014.
Roberts JA, Pea F, Lipman J. The clinical relevance of plasma protein binding changes. Clin Pharmacokinet. 2013;52:1–8.
Acknowledgments
The authors would like to thank Anjana Mallela and Vennila Dharman for their medical writing assistance with this manuscript.
This study was supported by Novartis Pharma AG, Basel, Switzerland.
Conflict of interest/disclosure
All authors are employees of Novartis, except for T. Majumdar who was employed by Novartis Pharma during the study conduct and manuscript development, and is currently employed by Alcon Laboratories, Inc.
Author information
Authors and Affiliations
Corresponding author
Additional information
Registered at ClinicalTrials.gov as NCT01594957.
Rights and permissions
About this article

Cite this article
Hirano, M., Meyers, D., Golla, G. et al. Effect of Hepatic Impairment on the Pharmacokinetics of Pradigastat, a Diacylglycerol Acyltransferase 1 (DGAT1) Inhibitor. Clin Pharmacokinet 54, 761–770 (2015). https://doi.org/10.1007/s40262-015-0235-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40262-015-0235-9