
Abstract
Introduction
Meta-analyses of observational studies represent an important tool for assessing efficacy and safety in the pharmacoepidemiologic field. The data from the individual studies are either primary (i.e., collected through interviews or self-administered questionnaires) or secondary (i.e., collected from databases that were established for other purposes). So far, the origin of the data (primary vs. secondary) has not been systematically assessed as a source of heterogeneity in pharmacoepidemiologic meta-analyses.
Objective
The aim was to assess the impact of considering the source of exposure data as a criterion in sensitivity and subgroup analysis on the conclusions of drug safety meta-analyses.
Methods
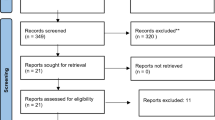
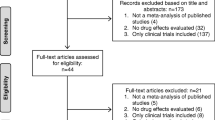
We selected meta-analyses published between 2013 and 2015 in which the intake of frequently used over-the-counter medicines was either the main exposure or a concomitant treatment and the outcome had short latency and induction periods. We stratified the results by origin of data (primary vs. secondary) and compared the new results to those presented originally in the meta-analyses.
Results
We used four meta-analyses that fulfilled our criteria of inclusion. The results were selective serotonin reuptake inhibitors and upper gastrointestinal bleeding: original estimate odds ratio (OR) = 1.71 [95% confidence interval (CI) 1.44–2.04], OR primary data = 1.19 (95% CI 0.90–1.58), OR secondary data = 1.81 (95% CI 1.50–2.17); proton pump inhibitors and cardiac events: original estimate hazard ratio (HR) = 1.35 (95% CI 1.18–1.54), HR primary data = 1.05 (95% CI 0.87–1.26), HR secondary data = 1.43 (95% CI 1.23–1.66); non-aspirin non-steroidal anti-inflammatory drugs and myocardial infarction: original estimate risk ratio (RR) = 1.08 (95% CI 0.95–1.22), RR primary data = 0.57 (95% CI 0.34–0.96), RR secondary data = 1.15 (95% CI 1.03–1.28); paracetamol during pregnancy and childhood asthma: original estimate OR = 1.32 (95% CI 1.14–1.52), OR primary data = 1.23 (95% CI 1.06–1.42), OR secondary data = 1.53 (95% CI 1.33–1.75).
Conclusions
The results after stratification are considerably modified. It is crucial to explore the origin of the data, either primary or secondary, as a source of heterogeneity in pharmacoepidemiologic meta-analyses to avoid misleading conclusions.




Similar content being viewed by others

References
Terris DD, Litaker DG, Koroukian SM. Health state information derived from secondary databases is affected by multiple sources of bias. J Clin Epidemiol. 2007;60:734–41.
Ray WA. Improving automated database studies. Epidemiology. 2011;22:302–4.
Schneeweiss S, Avorn J. A review of uses of health care utilization databases for epidemiologic research on therapeutics. J Clin Epidemiol. 2005;58:323–37.
Stoto MA. Drug safety meta-analysis: promises and pitfalls. Drug Saf. 2015;38:233–43.
Takkouche B, Khudyakov P, Costa-Bouzas J, et al. Confidence intervals for heterogeneity measures in meta-analysis. Am J Epidemiol. 2013;178:993–1004.
Egger M, Davey Smith G, Schneider M. Systematic reviews of observational studies. In: Egger M, Davey Smith G, Altman DG, editors. Systematic reviews in health care: meta-analysis in context. 2nd ed. London: BMJ Publishing Group; 2001. p. 211–27.
Petitti DB. Exploring heterogeneity. In: Petitti DB, editor. Meta-analysis, decision analysis, and cost-effectiveness analysis. Methods for quantitative synthesis in medicine. 2nd ed. New York: Oxford University Press; 2000. p. 213–227.
Madigan D, Ryan PB, Schuemie M, et al. Evaluating the impact of database heterogeneity on observational study results. Am J Epidemiol. 2013;178:645–51.
Jiang HY, Chen HZ, Hu XJ, et al. Use of selective serotonin reuptake inhibitors and risk of upper gastrointestinal bleeding: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2015;13:42–50.
Melloni C, Washam JB, Jones WS, et al. Conflicting results between randomized trials and observational studies on the impact of proton pump inhibitors on cardiovascular events when coadministered with dual antiplatelet therapy: systematic review. Circ Cardiovasc Qual Outcomes. 2015;8:47–55.
Varas-Lorenzo C, Riera-Guardia N, Calingaert B, et al. Myocardial infarction and individual nonsteroidal anti-inflammatory drugs meta-analysis of observational studies. Pharmacoepidemiol Drug Saf. 2013;22:559–70.
Hernández-Díaz S, Varas-Lorenzo C, García Rodríguez LA. Non-steroidal antiinflammatory drugs and the risk of acute myocardial infarction. Basic Clin Pharmacol Toxicol. 2006;98:266–74.
Cheelo M, Lodge CJ, Dharmage SC, et al. Paracetamol exposure in pregnancy and early childhood and development of childhood asthma: a systematic review and meta-analysis. Arch Dis Child. 2015;100:81–9.
Dickinson T, Malhi S, Painter S, et al. Association between SSRIs and upper gastrointestinal bleeding. Self treatment with non-steroidal drugs may be confounding factor. BMJ. 2000;20(320):1405.
Tougas G, Chen Y, Hwang P, et al. Prevalence and impact of upper gastrointestinal symptoms in the Canadian population: findings from the DIGEST study. Domestic/International Gastroenterology Surveillance Study. Am J Gastroenterol. 1999;94:2845–54.
Nagata N, Niikura R, Sekine K, et al. Risk of peptic ulcer bleeding associated with Helicobacter pylori infection, nonsteroidal anti-inflammatory drugs, low-dose aspirin, and antihypertensive drugs: a case-control study. J Gastroenterol Hepatol. 2015;30:292–8.
Tanskanen A, Tuomilehto J, Viinamäki H, et al. Joint heavy use of alcohol, cigarettes and coffee and the risk of suicide. Addiction. 2000;95:1699–704.
Brookhart MA, Rassen JA, Schneeweiss S. Instrumental variable methods in comparative safety and effectiveness research. Pharmacoepidemiol Drug Saf. 2010;19:537–54.
Glynn RJ, Schneeweiss S, Stürmer T. Indications for propensity scores and review of their use in pharmacoepidemiology. Basic Clin Pharmacol Toxicol. 2006;98:253–9.
Schneeweiss S. Sensitivity analysis and external adjustment for unmeasured confounders in epidemiologic database studies of therapeutics. Pharmacoepidemiol Drug Saf. 2006;15:291–303.
Gamble JM, McAlister FA, Johnson JA, et al. Quantifying the impact of drug exposure misclassification due to restrictive drug coverage in administrative databases: a simulation cohort study. Value Health. 2012;15:191–7.
U.S. Food and Drug Administration. Public Health Advisory: updated safety information about a drug interaction between clopidogrel bisulfate (marketed as Plavix) and Omeprazole (marketed as Prilosec and Prilosec OTC). November 17, 2009. http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm190787.htm. Accessed Dec 2016.
European Medicines Agency. Public statement on possible interaction between clopidogrel and proton pump inhibitors. May 29, 2009. http://www.ema.europa.eu/ema/index.jsp?curl=pages/news_and_events/news/2009/11/news_detail_000194.jsp&mid=WC0b01ac058004d5c1. Accessed Dec 2016.
Berlin JA, Golub RM. Meta-analysis as evidence: building a better pyramid. JAMA. 2014;312:603–6.
Lhachimi SK, Bala MM, Vanagas G. Evidence-based public health. Biomed Res Int. 2016;2016:5681409.
Holland WW. Health technology assessment and public health: a commentary. Int J Technol Assess Health Care. 2004;20:77–80.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Guillermo Prada-Ramallal, Bahi Takkouche and Adolfo Figueiras have no conflicts of interest that are directly relevant to the content of this study.
Funding
No sources of funding were used to assist in the preparation of this study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Prada-Ramallal, G., Takkouche, B. & Figueiras, A. Diverging Conclusions from the Same Meta-Analysis in Drug Safety: Source of Data (Primary Versus Secondary) Takes a Toll. Drug Saf 40, 351–358 (2017). https://doi.org/10.1007/s40264-016-0492-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-016-0492-z