
Abstract
Background
Previous studies have implicated the role of H. pylori infection in developing the metabolic syndrome. However, findings remain contradictory, and data from developing countries are scarce.
Methods
We employed a cross-sectional study design to assess the relationship between H. pylori infection and metabolic syndrome among diabetic patients attending Jimma Hospital, Ethiopia. An interviewer-led questionnaire administered to study participants provided information on sociodemographic factors, and medical records were used to obtain medical history information. Metabolic parameters, including plasma glucose, triglycerides (TG), high-density lipoprotein cholesterol (HDL-c), body-mass index (BMI), waist circumference (WC), systolic blood pressure (SBP), and diastolic blood pressure (DBP) were collected. H. pylori infection status was assessed using IgG Enzyme-linked Immunosorbent Assays (ELISA). The effect of H. pylori infection on metabolic syndrome and metabolic parameters was determined using multivariate linear and logistic regressions.
Results
We found H. pylori infection status was positively but not significantly associated with metabolic syndrome (AOR = 1.507, 95% CI: 0.570–3.981, p = 0.408). When the analysis was restricted to individual metabolic parameters, H. pylori positivity was significantly associated with lower HDL-c and higher SB, respectively.
Conclusions
Our result confirms that individual metabolic parameters, not an overall metabolic syndrome, are significantly associated with H. pylori infection. Future studies should examine the relationship between H. pylori and metabolic syndrome, considering gastrointestinal conditions such as GERD, GU, and DU.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Helicobacter pylori is a gram-negative bacterium affecting about 50% of the world’s population and is more prevalent in developing countries [1, 2]. A recent review of the global epidemiology of Helicobacter pylori in adults from 1970 to 2016 and children and adolescents from 2000 to 2021 indicated a consistently higher prevalence in Africa, the Eastern Mediterranean regions, and Middle and South America [3]. Moreover, a pooled analysis of H. pylori data involving 410,879 participants from 73 countries revealed variations in the prevalence of H. pylori by region, age, and sex, which are linked with different economic and social conditions [2].
H. pylori persistently inhabits the gastric mucosa in the absence of treatment [4] although the majority of those infected are asymptomatic. There is good evidence supporting the role of H. pylori in the development gastric and duodenal ulcer, distal gastric adenocarcinoma, peptic ulcer disease, and primary gastric mucosa associated lymphoid tissue (MALT) lymphoma [5, 6]. Given the ability of H. pylori virulence factors to modulate host immune response [7], there is growing interest in investigating the effects of H. pylori in extragastroduodenal diseases. A growing body of evidence has supported an association between H. pylori and extragastroduodenal diseases including cardiopulmonary, hematologic, neurologic, dermatologic, and metabolic diseases [8,9,10,11]. Our group in Ethiopia has found higher anemia prevalence, decreased growth trajectory, and reduced platelet indices among H. pylori-infected children compared with non-infected children [12,13,14], and provided supportive evidence for the potential role of H. pylori in extragastroduodenal diseases from a resource limited setting. However, these investigations didn’t explore the involvement of H. pylori in metabolic syndrome.
The potential association between H. pylori and metabolic syndrome is a topic of great interest as metabolic syndrome affects an estimated one-quarter of the world population, and it is becoming increasingly prevalent [15, 16]. Metabolic syndrome is defined by a variety of factors that predispose patients to greater risk of cardiovascular disease, type II diabetes, as well as significantly higher total mortality [17]. Metabolic parameters that predispose patients to developing metabolic syndrome include central obesity in addition to abnormal glucose levels, triglyceride levels, systolic blood pressure, diastolic blood pressure, as well as high-density lipoprotein and low-density lipoprotein cholesterol levels. Pervious clinical and epidemiological studies investigating the association between H. pylori infection status and prevalence of metabolic syndrome reported a positive association [18,19,20,21,22,23,24,25,26,27,28]. While two studies to date have found no such association [29, 30]. More recently, a meta-analysis conducted by Azami et al. suggests that collective findings overwhelmingly support a significant association between H. pylori infection and metabolic syndrome [8]. H. pylori infection has been linked to impaired insulin signaling in hepatocytes and increased expression of various inflammatory factors involved in developing insulin resistance [9]. Insulin resistance is a key factor associated with metabolic syndromes [31]. While metabolic syndrome is influenced by multiple genetic and environmental risk factors [32], proving the association between H. pylori and metabolic syndromes could make H. pylori one of the treatable causes of metabolic syndromes.
While previous epidemiological observations and mechanistic insights provide support for a role of H. pylori infection in metabolic syndrome development, most studies have been conducted in high-income populations, neglecting data from developing countries where the prevalence of H. pylori is greater [33]. Therefore, the aim of this study was to assess the relationship between H. pylori infection and metabolic syndrome, as well as the relationship between H. pylori infection and metabolic syndrome indicators including glucose, triglycerides, HDL-C, waist circumference, systolic blood pressure, and diastolic blood pressure. We therefore used clinical setting data from a developing country to assess the relationship between H. pylori infection and metabolic syndrome among diabetic patients attending Jimma Medical Center in Jimma, Ethiopia.
Methods
Study setting
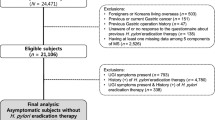
This study was conducted at Jimma Medical Center (JMC) in Jimma Town, Southwest Ethiopia. JMC is located in Jimma city, 352 km Southwest of Addis Ababa. Jimma, part of the Oromia region, sits at an elevation of 1780 m above sea level, and average daily temperatures range from 20 oC in July to 27 oC in January. The population of Jimma is estimated to be 208 000. Jimma Medical Center, comprised of 1600 staff members, provides service to a catchment population 15 million people, and is currently the only teaching and referral hospital in the southwestern part of Ethiopia. The chronic care clinic section of the center provides services for non-communicable diseases including hypertension and diabetes. Over three-thousand diabetic patients attend the diabetic follow up clinic, which runs twice weekly and provides integrated care for diabetic patients. Physicians, nurses, and final year medical and B Sc nursing students all provide diabetic services at the clinic. Data collection took place from August 15, 2020, to October 30, 2020. A convenience sampling technique was used to select 321 diabetic patients. We recruited patients attending the JMC chronic clinic that were over 18 years old. Patients who were critically ill, pregnant, unconscious, or had communication difficulties were excluded from the study. Patients who received antibiotics, proton pump inhibitors, H2 blockers, or bismuth treatment within one month prior to the study were also excluded.
Measurement and data collection
Questionnaires
Upon enrolling patients in this study, we then conducted structured questionnaires via face-to-face interviews, carried out by trained data collectors in the local language of patients, such as Afan Oromo or Amharic. These questionnaires were derived from the WHO stepwise approach to surveillance instruments, containing socio-demographic information, medical information, and modifiable risk factors such as smoking, alcohol consumption, khat chewing, fruit and vegetable consumption, type of oil used, and engagement in physical activity. Physical activity questionnaires were used to obtain data on the engagement of participants in physical activity in their daily lives. A participant engaging in greater than 150 min of moderate-intensity physical activity or greater than 75 min of high-intensity physical activity throughout the week, or greater than an equivalent combination of moderate- and high-intensity physical activity, was defined as physically active and labeled as “Yes”. Participants who did not meet this physically active definition criteria were defined as physically inactive and labeled as “No”. (Online supplementary information)
Anthropomorphic data
Anthropomorphic measurements including waist circumference (cm), weight (kg), and height (m) were measured, and body mass indices were computed as (weight (kg)) / [height (m)]2. All anthropomorphic measurements were performed by a trained data collector. Participants were instructed to remove their shoes, and digital scales were used to measure each participant’s weight. Standing height of shoeless participants was measured using a stadiometer. Waist circumference (WC) was measured around the midway portion between the lower border of the ribs and the bone crest at the widest portion over lightweight clothing using a soft tape measure, applying no pressure to the body.
Blood pressure data
A mercury-based sphygmomanometer was used to measure systolic blood pressure (SBP) and diastolic blood pressure (DBP). For blood pressure measurement, participants were instructed to lay and rest in a supine position for more than ten minutes, and then blood pressure measurements were obtained. Clinical data including but not limited to family history of diabetes, duration of diabetes, hypertension status, and medication for hypertension were obtained from patient self-reporting and analysis of personal health record files.
Blood sample collection and processing
Blood samples were taken from the antecubital vein of patients with minimal tourniquet time. After that, the punctured area was disinfected with 70% ethanol, and the samples were collected in a serum separator tube. Five milliliters (mL) of venous blood were collected after an overnight fast (8–12 h), and then transported to the clinical chemistry unit of the JMC laboratory for analysis. The blood specimens were held at room temperature for 20–30 min to facilitate clot formation, then centrifuged at 3000 rpm for five minutes to separate the serum from the blood. After separation, the serum samples were stored in Nunc tubes at -20 oC until analysis was performed.
Laboratory testing
All biochemical analyses were performed in the clinical chemistry unit of Jimma Medical Center Laboratory by the spectrophotometric method of the Cobas 6000 chemistry analyzer. Plasma glucose was determined by enzymatic hexokinase principle. Total cholesterol, high-density lipoprotein cholesterol (HDL-c), low-density lipoprotein (LDL-c), and triglycerides (TG) were determined by enzymatic colorimetric methods. From the same sample, H. pylori antibody levels were determined by the IgG Enzyme-linked Immunosorbent Assays (ELISA) method according to the manufacturer’s instructions. This was performed by the ELISA reader in the screening room at the Jimma blood bank laboratory. A patient was considered to be positive for.
H. pylori infection if the IgG anti H pylori antibody concentration was > 20 U/mL.
Data quality assurance
Questionnaires were prepared in English and translated to local language (Amharic and Afan Oromo). Data were collected by licensed laboratory technologist and nurses under the supervision of a principal investigator. To avoid mislabeling of samples, test tube labels were cross-checked with unique patient identification numbers. To ensure that specimens were free from hemolysis and lipemia, collected samples were visually checked. Blood samples were immediately processed and separated. All laboratory activities were completed according to standard operating procedures and reagents and instrumental equipment were thoroughly checked prior to analyzing patient samples.
Outcome and exposure variables
The primary study outcome was metabolic syndrome status. We defined metabolic syndrome according to modified International Diabetes Federation (IDF) criteria, present in Rafaeli et al. (2018) [26], which defined metabolic syndrome as two or more of the following conditions in addition to central obesity, defined as BMI ≥ 30 kg/m2: triglycerides ≥ 150 mg/dL, HDL < 40 mg/dL, plasma glucose ≥ 100 mg/dL. ‘Exposure to H. pylori infection’ was defined as a positive result provided by the ELISA reader.
Statistical analysis
Survey data and laboratory data from the JMC patient population was cleaned and coded for statistical analysis using IBM SPSS Statistics V.27. Before investigating the association between H. pylori infection and metabolic syndrome, univariate analyses were used to identify potential confounders. Variables associated with both the exposure (H. pylori infection) and outcome (metabolic syndrome status) variables in the crude analysis using a statistical significance cutoff of p < 0.3 were considered to be possible confounders. For our modified IDF definition of metabolic syndrome, these included family history of diabetes and coffee drinking status. The primary outcome of this analysis was metabolic syndrome status. Our hypothesis that H. pylori infection would be associated with metabolic syndrome status was assessed using univariate logistic regression to calculate a crude odds ratio and obtain a p value. Then multivariate logistic regression was performed, adding potential confounders to the model and then removing them according to the backward elimination technique. Additionally, we examined the relationship between H. pylori infection status and continuous variables (metabolic parameters) using univariate and multivariate generalized linear models. These variables included plasma glucose, triglycerides (TG), high-density lipoprotein cholesterol (HDL-c), body-mass index (BMI), waist circumference (WC), systolic blood pressure (SBP), and diastolic blood pressure (DBP). First, we analyzed the crude mean difference between H. pylori-positive and H. pylori-negative individuals, and then we repeated the analysis while adjusting for possible confounders, using the backwards elimination technique.
Results
Selected demographic characteristics and H. pylori infection status
A total of 321 patients were enrolled in this study. Of these participants, 62.6% (201/321) were male and a slight majority of 55.1% (177/321) lived in a rural area. The age range of the study population was 18–69 years and 29.3% (94/321) of participants were within the 60–69 years old range. The income range of the study participants spanned from no monthly income to monthly income ≥ 4000 Birr and 38% (122/321) reported having no monthly income. Analyzing education, 31.5% (101/321) of study participants had no formal education while 43.6% (140/321) of participants had received primary education. Most participants 85.4% (274) were married and 81.9% (263) reported regularly drinking coffee. The prevalence of H. pylori infection was 69.5% (223/321) (Table 1).
Metabolic syndrome components in study population
Of the entire study population, 8.4% (27/321) of participants were classified as having metabolic syndrome according to modified IDF criteria. All participants had glucose levels ≥ 100 mg/dL, and 59.5% (191/321) participants had triglycerides ≥ 150 mg/dL. Only 9% (29/321) of the population had elevated high-density lipoprotein (HDL-c) levels. Examining blood pressure, 42.7% of participants had elevated systolic blood pressure (SBP) ≥ 130 mmHg, and 22.7% (73/321) had elevated diastolic blood pressure (DBP) (Table 2).
Univariate analysis for relationships between potential confounders and H. pylori infection
The crude association between demographic variables and H. pylori infection was examined using univariate logistic regression. Univariate logistic regression was performed between demographic variables and metabolic syndrome status and then performed between demographic variables and H. pylori status to identify potential confounders. Family history of diabetes and coffee drinking status were found to be potential confounders in relation to the modified IDF definition of metabolic syndrome which is defined as two or more of the following conditions in addition to central obesity, defined as BMI ≥ 30 kg/m2: triglycerides ≥ 150 mg/dL, HDL < 40 mg/dL, plasma glucose ≥ 100 mg/dL. (Supplementary Tables 1 and 2). Interestingly, maternal education status, urban or rural residence, and age were not identified as significant confounders.
Association between H. Pylori infection and metabolic syndrome
In a multivariate logistic model between H. pylori status and metabolic syndrome status adjusted for potential confounders, patients infected with H. pylori showed higher odds of metabolic syndrome according to modified IDF criteria, yet results were not statistically significant (Adjusted odds Ratio (AOR) = 1.507, 95% CI: 0.570–3.981, p = 0.408) (Table 3).
Association between H. Pylori infection and metabolic syndrome-related outcomes
Linear regression models related plasma glucose, triglycerides, high-density lipoprotein cholesterol, body-mass index, waist circumference, systolic blood pressure, and diastolic blood pressure as continuous outcomes to the individual estimates of H. pylori status. These models showed significant increase in waist circumference among patients infected with H. pylori (mean difference: 4.337, 95% CI: 0.151–8.523, p = 0.042). These models also showed significant increase in systolic blood pressure among patients who were infected with H. pylori (mean difference: 4.867, 95% CI: 0.350–9.384, p = 0.035). When the analysis was adjusted for potential confounders found for JIS criteria, findings no longer remained statistically significant. When the analysis was adjusted for potential confounders using modified IDF criteria, there was a significant decrease in HDL-c observed among patients infected with H. pylori (adjusted mean difference: 6.651, 95% CI: 0.902–12.401, p = 0.024). Additionally, the increase in systolic blood pressure among H. pylori-infected patients remained significant when adjusting for confounders that were found using the IDF definition of metabolic syndrome (mean difference: 5.650, 95% CI: -11.278 - -0.22, p = 0.049) (Table 4).
Discussion
This study contributes to our understanding of the influence of H. pylori on metabolic syndrome status in diabetic patients in Ethiopia. We found H. pylori infection status was positively but not significantly associated with metabolic syndrome. We also found H. pylori positivity was significantly associated with lower HDL-c and higher SB, respectively.
Several other studies have examined the effects of H. pylori infection on various parameters of metabolic syndrome, and have found positive association between H. pylori with lower HDL-c levels [22,23,24], and higher systolic blood pressure [22]. These individual findings are supported by a meta-analysis conducted by Upala et al. (2016), which also found that, overall, H. pylori positivity is significantly associated with higher systolic blood pressure (p = 0.01) and lower HDL-c levels (p < 0.01) [34]. However, more recent cross-sectional studies in the United States of America and Iran have found no significant difference in HDL-c levels between H. pylori-positive and negative individuals [35,36,37].
In this study, our finding of no significant association between H. pylori infection and metabolic syndrome status is supported by few studies. Naja et al. (2012) and Takeoka et al. (2016) which also found that odds of metabolic syndrome did not significantly differ between H. pylori- positive and negative individuals, respectively [29, 30]. Similarly, Chen et al. (2019) found that H. pylori was not significantly associated with metabolic syndrome in females only [21]. However, this explanation disagrees with previous studies that have found an association between H. pylori infection and metabolic syndrome in apparently healthy populations [18,19,20,21,22,23,24,25,26,27,28]. In a meta-analysis conducted by Azami et al. (2021) showed a significant association between H. pylori positivity and metabolic syndrome with a pooled odds ratio of 1.19 (95% CI 1.05–1.35) [8]. The magnitude of the odds ratio from this result didn’t not materially different from our observations, although ours failed to reach statistically significant. This inconsistency could be due to variations in age, outcome ascertainment, and differences in the method used to assess H. pylori status.
Several hypotheses have been proposed regarding the mechanism by which H. pylori induces the development of metabolic syndrome. As H. pylori is known to disrupt gastric barrier function through the dysregulation of epithelial tight junctions [38], this predisposes the gut to mucosal damage [39]. It has been shown that mucosal damage induces the production of pro-inflammatory cytokines [7], which may affect glucose and lipid metabolism [40, 41], as these cytokines promote systemic inflammatory response [38, 42]. Interestingly, Mokhtar et al. found that H. pylori eradication in H. pylori-positive patients with functional dyspepsia resulted in a significant reduction of LDL levels, plasma glucose counts, and waist circumference Field [39], suggesting that H. pylori affects metabolic parameters and increased metabolic syndrome risk through interaction with the gastric epithelium. These findings are further substantiated by others who found that gastroesophageal reflux disease (GERD) and gastric ulcer (GU) Field [19], as well as a duodenal ulcer (DU) [26], were predictive for metabolic syndrome. Our failure to conclude a significant association between H. pylori positivity and metabolic syndrome may be explained by the lack of data on H. pylori-induced gastrointestinal abnormalities such as GU, DU, or GERD in the study population.
Our findings should be interpreted considering the following limitations. First, the cross-sectional design of our study makes it difficult to establish causal findings since we did not have patient data prior to H. pylori infection. Longitudinal studies are needed to improve our understanding of the effects of H. pylori infection. Similarly, H. pylori may be a symptom of other conditions, such as other infections or socioeconomic status. We collected demographic and lifestyle information using self-reported questionnaires, which may be susceptible to misclassification and recall bias. However, the questionnaire had previously been effective in a similar population in Ethiopia, increasing the validity of our findings. Furthermore, enrolling patients with known type I or type II diabetes mellitus introduces the possibility that diabetes status may be associated with H. pylori infection or metabolic syndrome. To account for these possibilities, we adjusted our findings for markers of socioeconomic status that had been significantly associated with the outcome variable (metabolic syndrome). A further potential limitation is our method of H. pylori detection. As we used the IgG Enzyme-linked Immunosorbent Assays (ELISA) method to diagnose H. pylori-positive individuals, Shin et al. (2012) found that serological detection methods were less sensitive than histological methods, and thus less capable of establishing a correlation between H. pylori and metabolic syndrome. However, no other studies have examined the association between H. pylori infection and metabolic syndrome using ELISA methods to detect H. pylori and ELISA methods have been proven to be a useful tool with high diagnostic performance in African settings [43]. Finally, the potential of reverse causality may also explain found associations between H. pylori and metabolic syndrome. However, H. pylori infection in developing countries such as Ethiopia frequently occurs early in life [44], which makes it unlikely that patient metabolic parameters abnormality preceded to H. pylori infection.
The definition of metabolic syndrome used for this study was another limitation of this study. We opted to use the modified International Diabetes Federation (IDF) criteria used by Rafaeli et al. (2018), which used a BMI cutoff of ≥ 30 kg/m2 as a proxy for determining central obesity as opposed to waist circumference values [26]. However, Body-mass index has been used as substitute for waist circumference because BMI and waist circumference have been found to be associated with BMI [45]. Although our study has limitations, this is the first study to investigate the potential link between H. pylori infection and metabolic syndrome in diabetic patients in Ethiopia. We gathered detailed lifestyle and demographic information to address potential confounding factors. We used comprehensive clinical laboratory data to define the study’s exposure and outcome objectively.
In conclusion, we found that H. pylori infection was significantly associated with lower levels of HDL-c and higher systolic blood pressure. However, we didn’t find a significant association between H. pylori infection status and overall metabolic syndrome. Future studies should seek to examine the relationship between H. pylori and metabolic syndrome in light of other gastrointestinal conditions.
Data availability
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Abbreviations
- MALT:
-
Mucosa Associated Lymphoid Tissue
- HDL-c:
-
High-Density Lipoprotein cholesterol
- LDL-c:
-
Low-Density Lipoprotein cholesterol
- TG:
-
Triglycerides
- GERD:
-
Gastroesophageal reflux disease
- BMI:
-
Body mass index
- IDF:
-
International Diabetes Federation
- GU:
-
Gastric Ulcer
- DU:
-
Duodenal Ulcer
- SBP:
-
Systolic Blood Pressure
- DBP:
-
Diastolic Blood Pressure
- WC:
-
Waist Circumference
- ELISA:
-
Enzyme-linked Immunosorbent Assays
References
Hooi JKY, Lai WY, Ng WK, Suen MMY, Underwood FE, Tanyingoh D, et al. Global prevalence of Helicobacter pylori infection: systematic review and Meta-analysis. Gastroenterology. 2017;153(2):420–9.
Zamani M, Ebrahimtabar F, Zamani V, Miller WH, Alizadeh-Navaei R, Shokri-Shirvani J, et al. Systematic review with meta-analysis: the worldwide prevalence of Helicobacter pylori infection. Aliment Pharmacol Ther. 2018;47(7):868–76.
Malfertheiner P, Camargo MC, El-Omar E, Liou JM, Peek R, Schulz C, et al. Helicobacter pylori infection. Nat Rev Dis Primers. 2023;9(1):19.
Blaser MJ, Atherton JC. Helicobacter pylori persistence: biology and disease. J Clin Invest. 2004;113(3):321–33.
Atherton JC. The pathogenesis of Helicobacter pylori-induced gastro-duodenal diseases. Annu Rev Pathol. 2006;1:63–96.
Graham DY. Helicobacter pylori update: gastric cancer, reliable therapy, and possible benefits. Gastroenterology. 2015;148(4):719–e313.
White JR, Winter JA, Robinson K. Differential inflammatory response to Helicobacter pylori infection: etiology and clinical outcomes. J Inflamm Res. 2015;8:137–47.
Azami M, Baradaran HR, Dehghanbanadaki H, Kohnepoushi P, Saed L, Moradkhani A, et al. Association of Helicobacter pylori infection with the risk of metabolic syndrome and insulin resistance: an updated systematic review and meta-analysis. Diabetol Metab Syndr. 2021;13(1):145.
Polyzos SA, Kountouras J, Zavos C, Deretzi G. The association between Helicobacter pylori infection and insulin resistance: a systematic review. Helicobacter. 2011;16(2):79–88.
Vaira U, Gatta L, Ricci C, D’Anna L, Iglioli MM. Helicobacter pylori: diseases, tests and treatment. Dig Liver Dis. 2001;33(9):788–94.
Wong F, Rayner-Hartley E, Byrne MF. Extraintestinal manifestations of Helicobacter pylori: a concise review. World J Gastroenterol. 2014;20(34):11950–61.
Baxendell K, Walelign S, Tesfaye M, Wordofa M, Abera D, Mesfin A, et al. Association between infection with Helicobacter pylori and platelet indices among school-aged children in central Ethiopia: a cross-sectional study. BMJ Open. 2019;9(4):e027748.
Taye B, Enquselassie F, Tsegaye A, Amberbir A, Medhin G, Fogarty A, et al. Effect of early and current Helicobacter pylori infection on the risk of anaemia in 6.5-year-old Ethiopian children. BMC Infect Dis. 2015;15:270.
Taye B, Enquselassie F, Tsegaye A, Amberbir A, Medhin G, Fogarty A, et al. Effect of Helicobacter pylori infection on growth trajectories in young Ethiopian children: a longitudinal study. Int J Infect Dis. 2016;50:57–66.
Cameron AJ, Shaw JE, Zimmet PZ. The metabolic syndrome: prevalence in worldwide populations. Endocrinol Metab Clin North Am. 2004;33(2):351–75. table of contents.
Giudice A, Crispo A, Massimiliano G, D’Arena G, Tecce MF, Grimaldi M, et al. Metabolic syndrome, insulin resistance, circadian disruption, antioxidants and pancreatic carcinoma: an overview. J Gastrointestin Liver Dis. 2014;23(1):73–7.
Malik S, Wong ND, Franklin SS, Kamath TV, L’Italien GJ, Pio JR, et al. Impact of the metabolic syndrome on mortality from coronary heart disease, cardiovascular disease, and all causes in United States adults. Circulation. 2004;110(10):1245–50.
Chen LW, Chien CY, Hsieh CW, Chang LC, Huang MH, Huang WY, et al. The associations between Helicobacter pylori infection, serum vitamin D, and metabolic syndrome: a community-based study. Med (Baltim). 2016;95(18):e3616.
Chen LW, Chien CY, Yang KJ, Kuo SF, Chen CH, Chien RN. Helicobacter pylori infection increases insulin resistance and metabolic syndrome in residents younger than 50 Years Old: A Community-based study. PLoS ONE. 2015;10(5):e0128671.
Chen TP, Hung HF, Chen MK, Lai HH, Hsu WF, Huang KC, et al. Helicobacter Pylori Infection is positively Associated with metabolic syndrome in Taiwanese adults: a cross-sectional study. Helicobacter. 2015;20(3):184–91.
Chen YY, Fang WH, Wang CC, Kao TW, Chang YW, Wu CJ, et al. Helicobacter pylori infection increases risk of incident metabolic syndrome and diabetes: a cohort study. PLoS ONE. 2019;14(2):e0208913.
Gunji T, Matsuhashi N, Sato H, Fujibayashi K, Okumura M, Sasabe N, et al. Helicobacter pylori infection is significantly associated with metabolic syndrome in the Japanese population. Am J Gastroenterol. 2008;103(12):3005–10.
Lim SH, Kim N, Kwon JW, Kim SE, Baik GH, Lee JY, et al. Positive Association between Helicobacter pylori Infection and metabolic syndrome in a Korean Population: a Multicenter Nationwide Study. Dig Dis Sci. 2019;64(8):2219–30.
Lu LJ, Hao NB, Liu JJ, Li X, Wang RL. Correlation between Helicobacter pylori Infection and Metabolic Abnormality in General Population: a cross-sectional study. Gastroenterol Res Pract. 2018;2018:7410801.
Nabipour I, Vahdat K, Jafari SM, Pazoki R, Sanjdideh Z. The association of metabolic syndrome and Chlamydia pneumoniae, Helicobacter pylori, cytomegalovirus, and herpes simplex virus type 1: the Persian Gulf Healthy Heart Study. Cardiovasc Diabetol. 2006;5:25.
Refaeli R, Chodick G, Haj S, Goren S, Shalev V, Muhsen K. Relationships of H. Pylori infection and its related gastroduodenal morbidity with metabolic syndrome: a large cross-sectional study. Sci Rep. 2018;8(1):4088.
Shin DW, Kwon HT, Kang JM, Park JH, Choi HC, Park MS, et al. Association between metabolic syndrome and Helicobacter pylori infection diagnosed by histologic status and serological status. J Clin Gastroenterol. 2012;46(10):840–5.
Yu Y, Cai J, Song Z, Wang J, Wu L. Association of Helicobacter pylori infection with metabolic syndrome in aged Chinese females. Exp Ther Med. 2019;17(6):4403–8.
Naja F, Nasreddine L, Hwalla N, Moghames P, Shoaib H, Fatfat M, et al. Association of H. Pylori infection with insulin resistance and metabolic syndrome among Lebanese adults. Helicobacter. 2012;17(6):444–51.
Takeoka A, Tayama J, Yamasaki H, Kobayashi M, Ogawa S, Saigo T, et al. Impact of Helicobacter pylori Immunoglobulin G Levels and atrophic gastritis status on risk of metabolic syndrome. PLoS ONE. 2016;11(11):e0166588.
Roberts CK, Hevener AL, Barnard RJ. Metabolic syndrome and insulin resistance: underlying causes and modification by exercise training. Compr Physiol. 2013;3(1):1–58.
Gosadi IM. Assessment of the environmental and genetic factors influencing prevalence of metabolic syndrome in Saudi Arabia. Saudi Med J. 2016;37(1):12–20.
Amberbir A, Medhin G, Erku W, Alem A, Simms R, Robinson K, et al. Effects of Helicobacter pylori, geohelminth infection and selected commensal bacteria on the risk of allergic disease and sensitization in 3-year-old Ethiopian children. Clin Exp Allergy. 2011;41(10):1422–30.
Upala S, Jaruvongvanich V, Riangwiwat T, Jaruvongvanich S, Sanguankeo A. Association between Helicobacter pylori infection and metabolic syndrome: a systematic review and meta-analysis. J Dig Dis. 2016;17(7):433–40.
Eslami O, Shahraki M, Shahraki T, Ansari H. Association of Helicobacter pylori infection with metabolic parameters and dietary habits among medical undergraduate students in southeastern of Iran. J Res Med Sci. 2017;22:12.
Gillum RF. Infection with Helicobacter pylori, coronary heart disease, cardiovascular risk factors, and systemic inflammation: the Third National Health and Nutrition Examination Survey. J Natl Med Assoc. 2004;96(11):1470–6.
Sotuneh N, Hosseini SR, Shokri-Shirvani J, Bijani A, Ghadimi R. Helicobacter pylori infection and metabolic parameters: is there an association in elderly population? Int J Prev Med. 2014;5(12):1537–42.
Wroblewski LE, Shen L, Ogden S, Romero-Gallo J, Lapierre LA, Israel DA, et al. Helicobacter pylori dysregulation of gastric epithelial tight junctions by urease-mediated myosin II activation. Gastroenterology. 2009;136(1):236–46.
Marcus EA, Vagin O, Tokhtaeva E, Sachs G, Scott DR. Helicobacter pylori impedes acid-induced tightening of gastric epithelial junctions. Am J Physiol Gastrointest Liver Physiol. 2013;305(10):G731–9.
Albaker WI. Helicobacter pylori infection and its relationship to metabolic syndrome: is it a myth or fact? Saudi J Gastroenterol. 2011;17(3):165–9.
Aslan M, Nazligul Y, Horoz M, Bolukbas C, Bolukbas FF, Gur M, et al. Serum paraoxonase-1 activity in Helicobacter pylori infected subjects. Atherosclerosis. 2008;196(1):270–4.
Chmiela M, Gonciarz W. Molecular mimicry in Helicobacter pylori infections. World J Gastroenterol. 2017;23(22):3964–77.
Tshibangu-Kabamba E, Phuc BH, Tuan VP, Fauzia KA, Kabongo-Tshibaka A, Kayiba NK, et al. Assessment of the diagnostic accuracy and relevance of a novel ELISA system developed for seroepidemiologic surveys of Helicobacter pylori infection in African settings. PLoS Negl Trop Dis. 2021;15(9):e0009763.
Jaganath D, Saito M, Gilman RH, Queiroz DM, Rocha GA, Cama V, et al. First detected Helicobacter pylori infection in infancy modifies the association between diarrheal disease and childhood growth in Peru. Helicobacter. 2014;19(4):272–9.
Ford ES, Mokdad AH, Giles WH. Trends in waist circumference among U.S. adults. Obes Res. 2003;11(10):1223–31.
Acknowledgements
We thank the study participants in who generously provided information, and the Jimma medical center (JMC) laboratory staffs and JMC chronic clinic for their full cooperation, assistance in the provision of required information. We also grateful to to Jimma blood bank for allowing us to use the laboratory space and instruments to the ELISA test. We also thank Colgate University Research Council for providing ELISA test kits to detect H.pylori The views expressed are those of the authors and not necessarily those of the Colgate University , or Jimma University.
Funding
Funding for H. pylori ELISA analysis provided by Colgate University Research Council. TI was supported by Jimma University to collect data collection as part of his graduate training.
Author information
Authors and Affiliations
Contributions
BT conceived and designed the study, and critically reviewed the manuscript. TI participated in the study design, data collection, and analysis, and drafted the initial manuscript. WC supervised the field data collection and critically reviewed the manuscript. WR, AG, and EZ assisted in data analysis and interpretation and critically reviewed the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Institutional Review Board (IRB) of Jimma University, Ethiopia approved the study. Informed consent was obtained from each patient before recruitment after explaining the study’s objectives in the language they understood. The patients were informed that participation in the study would be voluntary and free. They were also informed that refusing or withdrawing from the study wouldn’t jeopardize their right to receive any services. To ensure participant privacy, confidential numerical identifiers are assigned to each study subject, and all participant information remains password protected in electronic files. All methods were carried out in accordance with the relevant ethical guidelines and regulations of the Jimma University Institutional Review Board (IRB).
Consent for publication
All study subject enrolled in the study have provided their informed consent for the publication of the research results. In line with the IRB guide ethical guidelines and regulations all personal data or identifiable information were anonymized to protect individual privacy.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ibrahim, T., Russel, W., Getachew, A. et al. Association between infection with Helicobacter pylori and metabolic syndrome among diabetic patients attending Jimma medical center in Jimma city, Ethiopia: a cross-sectional study. BMC Infect Dis 24, 922 (2024). https://doi.org/10.1186/s12879-024-09840-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09840-w