
Abstract
Background
Acute-on-chronic liver failure (ACLF) is characterized by a systemic inflammatory response, predominantly associated with hepatitis B virus in the Asia-Pacific region, with a high short-term mortality rate. The platelet to high-density lipoprotein ratio (PHR) has been used to predict the prognosis of patients with various inflammatory diseases. We aim to is to use the PHR to predict the short-term prognosis of patients with HBV-ACLF.
Method
In this study, we retrospectively analyzed clinical data from 270 HBV-ACLF patients. Using logistic regression, we identified independent risk factors for short-term mortality and developed a prognostic model. This model was then validated, compared, and its clinical utility assessed via decision curve analysis (DCA).
Results
Among the 270 HBV-ACLF patients, 98 patients died within 28 days. The deceased group exhibited a higher proportion of severe hepatic encephalopathy and ascites. Additionally, there was a statistically significant difference (P = 0.046) in the novel inflammation scoring system, PHR, between the two groups. Following stringent variable selection, PHR was identified as a predictive factor for short-term mortality in HBV-ACLF patients using logistic regression analysis (OR: 0.835 (0.756–0.999), P = 0.009), and it exhibited a synergistic effect with certain traditional scores. The prognostic model constructed based on PHR demonstrated a superior ability to predict short-term mortality compared to traditional scores such as Child-Turcotte-Pugh (AUC: 0.889). Evaluation using calibration curves and decision curve analysis (DCA) suggested its practical utility.
Conclusion
PHR can predict short-term mortality in patients, with a low PHR upon admission being associated with an increased risk of death.
Similar content being viewed by others


Introduction
Acute-on-chronic liver failure (ACLF) is characterized by an acute deterioration of liver function, manifesting as jaundice, coagulation dysfunction, and the occurrence of ascites, with a high 28-day mortality rate [1]. More than a quarter of patients with cirrhosis present with this condition upon admission [1, 2]. In the Asia-Pacific region, including China, chronic hepatitis B virus (HBV) infection is the primary cause of ACLF, accounting for over 60% of ACLF cases [3]. Currently, there is a lack of specific treatment for ACLF, and the main approaches involve managing precipitating events, organ support, and liver transplantation. Nonetheless, under specific monitoring conditions, the 28-day and 90-day mortality rates for ACLF patients are 37.6% and 50.4%, respectively [4]. Therefore, early diagnosis and understanding of prognosis are crucial means to improve patient survival.
Systemic inflammation is a characteristic pathophysiological feature of ACLF [1]. In fact, Alberto and his colleagues reported that the severity of inflammation, rather than coagulation dysfunction, is the most important predictor of ACLF [5]. The inflammation score based on simple laboratory test indicators, such as monocyte-to-lymphocyte ratio (MLR) [6], neutrophil-lymphocyte ratio (NLR) [7], and lymphocyte-to-white blood cell ratio (LWR) [8], is used to predict the prognosis of patients with liver failure or cirrhosis. However, the need to explore further the potential of inflammatory scoring for predicting the prognosis of patients with ACLF caused by specific etiologies has not been met yet.
The platelet to high-density lipoprotein cholesterol ratio (PHR) is a newly developed systemic inflammation marker, reported as a biomarker for patient prognosis in metabolic syndrome [9] and non-alcoholic fatty liver disease [10]. Interestingly, platelets serve as predictive factors in patients with cirrhosis [11, 12], while high-density lipoprotein (HDL) is associated with immunity [13] and has also been reported as a predictive factor in decompensated cirrhotic patients [14]. However, there is currently a lack of practical data on the association between PHR and the prognosis of ACLF patients, especially hepatitis B virus-related acute-on-chronic liver failure (HBV-ACLF) patients.
In this study, we employed data from HBV-ACLF patients at our center to explore the potential association between PHR and their prognosis. Additionally, we developed a new prognostic model based on PHR to predict the prognosis of patients within 28 days.
Method
Study design and population
This retrospective study included 270 HBV-ACLF patients who were hospitalized at the First Affiliated Hospital of Nanchang University from April 2021 to March 2023. By analyzing the clinical data of this cohort, we aim to explore the correlation between systemic inflammation-related biomarkers and the 28-day mortality among patients. Patients with HBV-ACLF were recruited according to Asia Pacific Association for study of Liver (APASL) criteria [15], which required HBsAg positivity for at least 6 months, a serum total bilirubin (TBIL) level of 5 mg/dL or higher, an INR level of 1.5 or higher, or a prothrombin activity level of less than 40%, and the development of ascites and/or hepatic encephalopathy within 4 weeks. In general, patients were included when they met following criteria: (1) ≥ 18 years old, (2) diagnosed with HBV-ACLF, (3) no previous use of anti-lipid drugs and (4) clinical information is available. Exclusion criteria included (1) hepatocellular carcinoma, (2) combined with other chronic liver disease, (3) previous liver transplantation, (4) complications with other severe chronic extrahepatic diseases, (5) infection was known to have occurred before admission, and (6) infection with HIV or receiving immune-suppressive medication. Figure 1 depicts the flowchart of the study. Our study was approved by the Ethics Committee of the First Affiliated Hospital of Nanchang University (IIT [2021] 09). Informed consents of the patients were waived by the Ethics Committee of the First Affiliated Hospital of Nanchang University because of the retrospective and anonymous nature of the study. All relevant statements involving human subjects comply with the Declaration of Helsinki.

Design diagram of this study
Clinical data
A retrospective review of history, physical examinations, and laboratory measurements will be extracted from the inpatient information management system. Necessary laboratory measurements must be measured within 24 h of admission to meet the requirements. Clinical indicators include blood routine examination, liver function tests, renal function tests, coagulation function tests, blood lipid levels, and serum hepatitis B virus DNA (HBV-DNA). Finally, the survival status of the patients at 28 days will be meticulously documented.
Management and treatment
The management of patients with HBV-ACLF is based on established guidelines [2, 15], primarily the Acute-on-chronic liver failure: consensus recommendations of APASL (2019 edition) and the Chinese Guidelines for the Diagnosis and Management of Liver Failure (2018 edition). All patients with HBV-ACLF receive standardized medical treatment during hospitalization, including rest, fluid balance, nutritional support, and the use of nucleotide analogs. The intake of hepatotoxic substances or alcohol is required to be immediately discontinued. Patients are restricted in sodium and water intake and are treated with diuretics. Paracentesis is performed according to the severity of ascites and other specific patient conditions. For patients with bacterial infections, empirical antibiotic treatment is initiated, and subsequently adjusted based on culture and antibiotic sensitivity test results. In cases of hepatic encephalopathy (HE), precipitating factors are addressed simultaneously with medication, primarily consisting of lactulose, branched-chain amino acids, and ornithine aspartate.
Statistical analysis
Continuous variables were presented using means and standard deviations (SD) or medians and interquartile ranges (IQR), while categorical variables were represented using frequencies (%). We examined whether there were interactions between explanatory variables, such as variance inflation factors (VIF) and variable correlations, and found no significant interactions among the variables considered. Group comparisons were conducted using Student’s t-test or Mann-Whitney U test. The diagnostic accuracy of different models was evaluated through Receiver Operating Characteristic (ROC) analysis. ROC curve area under the curve (AUC) was compared following the method described by DeLong et al. All statistical tests were two-tailed with a significance level set at 5%. All analyses were performed using R 4.1.0 (R Project for Statistical Computing, Vienna, Austria). R packages used for model building and statistical analysis included gtsummary, tidyverse, performance, ggcorrplot, pROC, rms, and compareGroups. The source file “stdca.r” obtained from www.mskcc.org was used to generate Decision Curve Analysis (DCA) plots.
Result
Clinical characteristics
This study retrospective analysis a total of 270 HBV-ACLF patients who met the criteria for the APASL, among whom 98 (36.3%) patients died within 28 days. Those patients had a mean age of 49.2 ± 12.4 years and exhibited significant abnormalities in both coagulation function and liver function. Most patients did not present with hepatic encephalopathy at the time of admission, while nearly half of the patients had a small amount of ascites upon admission. Liver function scores for these patients were assessed at admission, including Child-Turcotte-Pugh (CTP) score, Model for end-stage liver disease (MELD) score, MELD sodium (MELD-Na) score, and Chinese Group on the Study of Severe Hepatitis B-ACLF II score (COSSHACLF IIs), which were 11.0 (10.0–12.0), 21.0 (17.4–24.8), 21.2 (17.5–26.9), and 6.81 (6.22–7.70), respectively. Additionally, we calculated a biomarker reflecting systemic inflammation, the PHR, which had a median value of 439 (258–789) in this cohort. Other baseline characteristics are described in Table 1.
Differences in characteristics between the survival and the death groups
Figure 2 provides a visual comparison of liver function scores and PHR scores between the survival and death groups, which indicates that the non-survival group had higher liver function scores and lower PHR scores. Specifically, the death group exhibited a higher proportion of male patients, along with elevated levels of PT, INR, MAP, WBC, TBIL, AST, HBV-DNA, and a higher incidence of severe HE. However, these patients had lower levels of cholesterol and triglycerides, as well as lower serum sodium levels. The comparison of baseline characteristics and corresponding p-values are presented in Table 1.

Box plots of various indicators for the survival and death groups. A: Comparison of CTP in the survival and death group at 28 days. B: Comparison of MELD in the survival and death group at 28 days. C: Comparison of MELD-Na in the survival and death group at 28 days. D: Comparison of COSSH-ACLF IIs in the survival and death group at 28 days. E: Comparison of PHR in the survival and death group at 28 days
Development of prognostic model for prediction of survival
Univariate regression analysis and multivariable regression analysis were used to identify independent risk factors for 28-day mortality rate in patients. Firstly, Gender, Age, INR, PT, MAP, TBIL, AST, BUN, Cholesterol, sNa, HBV-DNA, HBeAg, and PHR were identified as independent predictive factors. To avoid multicollinearity among variables, a correlation test between the variables was conducted to exclude variables that showed strong correlations from the multivariable regression analysis (Supplementary Fig. 1). VIF were also used to assess the multicollinearity among variables in the model. As shown in Supplementary Fig. 2, the VIF values of the variables included in the multivariable regression analysis were within a reasonable range. Finally, we identified Gender (OR: 0.16, 95% CI: 0.05–0.51, P = 0.003), Age (OR: 1.07, 95% CI: 1.04–1.12, P < 0.001), PT (OR: 1.1, 95% CI: 1.05–1.16, P < 0.001), MAP (OR: 1.04, 95% CI: 1.01–1.07, P = 0.018), WBC (OR: 1.23, 95% CI: 1.08–1.40, P = 0.001), TBIL (OR:1.01, 95% CI: 1.00-1.01, P < 0.001), log10DNA (OR:1.61, 95% CI: 1.28–2.06, P < 0.001), and PHR (OR: 0.835, 95% CI: 0.756–0.999, P = 0.009) as independent predictive factors (Table 2).
Validation and comparison of predictive model
Based on the above results, the specific formula for the predictive model is as follows: Predictive Model = -1.914 * Gender + 0.086 * Age + 0.093 * PT + 0.035 * MAP + 0.218 * WBC + 0.006 * TBIL + 0.5115 * log10DNA − 0.001 * PHR − 14.775. In the first step, we constructed the confusion matrix which used to evaluate the performance of our prediction model. The detailed parameters are as follows: Accuracy of 0.8370, Precision of 0.8855, Specificity of 0.8698, Recall of 0.8547, and F1 Score of 0.867 (refer to Fig. 3). Then we validated the model with calibration curve and discrimination analysis. The calibration curve indicated that the model had good predictive accuracy, while the probability curve suggested that the model could effectively differentiate between patients in the survival and death groups (refer to Fig. 4).

Parameters of the prognostic model. A, B and C: Confusion matrix of the prognostic mode

Validation of the prognostic model. A: Calibration curve of the prognostic model. B: Probability-Actual Outcome Curve
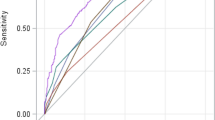
We further compared the predictive performance of the developed model with that of commonly used models by conducting a comparison of the area under the receiver operating characteristic curve (AUC) and performing the DeLong test. In summary, the newly developed model exhibits significantly higher predictive capability compared to the traditional CTP classification, MELD score, and MELD-Na score. However, when compared to the COSSH ACLF II score developed specifically for HBV-ACLF patients, there is no statistically significant difference (refer to Fig. 5; Table 3).

AUROC analysis of the prognostic model. The AUROC of (A) CTP, (B) MELD, (C) MELD-Na and (D) COASS-ACLF IIs comparison with the prognostic model, statistical comparison using the DeLong method
Clinical utility analysis
Decision curve analysis (DCA) is a suitable approach for evaluating predictive models by assessing net benefits across a range of threshold probabilities. It can identify risk models and assist us in making better clinical decisions. As shown in Fig. 6, the prognostic model based on PHR demonstrates superior clinical decision-making performance compared to traditional CTP score, MELD score, and MELD-Na score.

Clinical utility analysis. DCA curves of different prognostic models
The correlation between biomarkers and existing prognostic scores not only demonstrates the accuracy of biomarker prediction capabilities but also indicates the redundancy or overlap with existing models. If biomarkers can identify individuals who are classified as low-risk by traditional prognostic scoring but are actually at high risk, they would further demonstrate their predictive value and complement the existing prognostic scoring systems. Therefore, we correlated PHR with four widely recognized prognostic scores. As shown in Supplementary Fig. 3, the correlation between PHR and CTP grading is statistically significant with a P-value of 0.003, indicating the predictive consistency of PHR for liver classification in patients. However, there was no significant correlation between PHR and MELD score, MELD-Na score, and COSSH-ACLF II score. This suggests that under the same MELD score, MELD-Na score, or COSSH-ACLF II score, prognosis stratification based on PHR levels can provide additional predictive value for patient outcomes.
Discussion
One of the means to alleviate the burden on public health is the early assessment of patients’ prognosis, guiding clinical management, and providing personalized care. Systemic inflammation is a major driving factor of ACLF and a significant pathophysiological characteristic of ACLF [1, 2, 4]. In this explorative study, we conducted the first evaluation of the association between the systemic inflammation score PHR and the prognosis of HBV-ACLF. We found a negative correlation between PHR levels and liver function in patients, with lower PHR levels observed in patients with poorer prognosis. Further regression analysis revealed that PHR was an independent risk factor for the 28-day mortality rate of patients. The prognostic performance of the score constructed based on PHR levels was significantly higher than that of CTP score, MELD score, and MELD-Na score. DCA also indicated that the newly developed prognostic score had higher clinical utility than traditional scores.
Several simple, accurate, and objective inflammatory scores have been used for predicting specific inflammatory-related disease spectra, with the most common being NLR. It exhibits excellent predictive abilities in sepsis [16], organ transplantation [17], stroke [18], cancer [19], and liver failure [7, 20] by accurately forecasting disease progression and identifying patient prognosis. The promising clinical utility of these user-friendly systemic inflammatory scores is demonstrated, highlighting their potential value in clinical practice. In fact, the inflammatory score, PHR, also originates from common laboratory indicators and was initially identified to be associated with metabolic syndrome [9]. It is a syndrome characterized by endothelial dysfunction, inflammation, and the release of procoagulant mediators. Chun Feng et al. further investigated the relationship between PHR and liver fibrosis using a large sample cohort, and suggested that PHR could serve as a marker for liver fibrosis [10]. The close association of PHR with inflammation and fibrosis makes it a potential novel biomarker for identifying the prognosis of HBV-ACLF patients in the context of cirrhosis.
Thrombocytopenia is a prominent feature of chronic liver disease and cirrhosis [21]. It has been traditionally believed that excessive platelet clearance is due to splenic hyperfunction caused by portal hypertension. Recent studies, however, have shown a decrease in platelet production and functional defects in platelets [21, 22]. The study by Wang et al. has reported that platelet count is an independent predictor of survival in patients with HBV-ACLF [23]. In patients with liver cirrhosis, platelet count is also one of the predictors of decompensation [24]. In patients with liver cirrhosis, platelet count is also one of the predictors of decompensation [24]. In our cohort, the platelet count of patients in the deceased group was slightly lower than that of the survival group, although not statistically significant. However, in terms of white blood cell count, the level in the deceased group was significantly higher than that in the survival group. The potential mechanism may involve an increased degree of platelet-leukocyte aggregation in HBV-ACLF patients, promoting immune dysregulation in the body [25]. This is because platelet-induced leukocyte activation is enhanced, and ongoing platelet activation may also contribute to an increased formation of platelet-leukocyte complexes [25, 26]. Unfortunately, this study did not measure markers of platelet activation, and further research is needed to confirm this hypothesis.
Another parameter in PHR is high-density lipoprotein cholesterol. HDL-C is not only involved in lipid metabolism but also serves as an indicator of immune function in inflammatory diseases. HDL-C possesses various protective functions such as anti-infection, anti-inflammatory, antioxidant, anti-thrombotic, and immune-regulatory properties [13, 27]. Indeed, Markus and his colleagues have found that HDL-C is a reliable predictor of survival in patients with chronic liver failure [28]. Our team has also discovered that low levels of HDL-C can predict poor prognosis in patients with HBV-ACLF [29]. In our cohort, we also confirmed the above results. When comparing between groups, the levels of HDL-C in the deceased group were lower than those in the survival group. Mechanistically, HDL-C can bind to LPS in the blood, reducing inflammatory responses [30]. On the other hand, it regulates inflammasome function to decrease the maturation of pro-inflammatory cytokines [13]. Platelet count and HDL-C alone are not independent risk factors for HBV-ACLF patients. In fact, the PHR is considered a systemic inflammation score and has some correlation with liver fibrosis. It is explainable that the prognosis of ACLF patients with a cirrhotic background, characterized by a systemic inflammatory response, can be represented by this score.
In addition, in our cohort, the COSSH-ACLF II score [31] developed by a Chinese research team demonstrates comparable predictive capability to our developed prognostic model (AUC: 0.874 vs. 0.889, P = 0.459), suggesting that our prognostic model is non-inferior to COSSH-ACLF IIs. Furthermore, through a correlated analysis between patients’ PHR levels and COSSH-ACLFIIs, we found no significant correlation between the two. This implies that at the same COSSH-ACLFIIs, calculating the PHR can further stratify patients for their 28-day prognosis, as PHR also serves as an independent predictor of short-term mortality.
This study has the following limitations. Firstly, it is a single-center retrospective clinical data analysis, inevitably leading to potential biases. However, we have mitigated its impact on the results by employing diverse statistical analyses. Secondly, this study lacks external validation using independent datasets. We only conducted calibration curve analysis through 1000 resamplings and actual probability-prediction probability curve analysis to collectively assess the predictive model’s accuracy. Finally, we excluded patients who had been consistently using lipid-lowering drugs, and caution should be exercised in applying the obtained results to this subgroup.
In conclusion, our study indicates that PHR is an independent risk factor for short-term mortality in HBV-ACLF patients. The clinical prediction model built based on PHR exhibits significantly improved accuracy in predicting 28-day mortality compared to traditional prognostic scores. PHR may serve as a simple and accurate biomarker for short-term mortality in HBV-ACLF patients.
Data availability
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- INR:
-
International Normalized Ratio
- PT:
-
Prothrombin Time
- MAP:
-
Mean Artery Pressure
- TBIL:
-
Total Bilirubin
- ALT:
-
Alanine Aminotransferase
- AST:
-
Aspartate Aminotransferase
- ALP:
-
Alkaline Phosphatase
- GGT:
-
Glutamyl Transpeptidase
- sCr:
-
Serum Creatinine
- BUN:
-
Blood Urea Nitrogen
- HDL:
-
High-Density Lipoprotein
- LDL:
-
Low-Density Lipoprotein
- sNa:
-
Serum Sodium
- HBeAg:
-
Hepatitis B virus e Antigen
- CTP:
-
Child-Turcotte-Pugh
- MELD:
-
Model for End-stage Liver Disease
- MELD-Na:
-
MELD Sodium
- COSSH-ACLF IIs:
-
Chinese Group on the Study of Severe Hepatitis B-ACLF II score
- PHR:
-
Platelet /HDL ratio
References
MOREAU R, GAO B, PAPP M, et al. Acute-on-chronic liver failure: a distinct clinical syndrome [J]. J Hepatol. 2021;75(Suppl 1):S27–35.
HERNAEZ R, SOLà E, MOREAU R, et al. Acute-on-chronic liver failure: an update [J]. Gut. 2017;66(3):541–53.
ZHANG Y, TAN W, WANG X, et al. Metabolic biomarkers significantly enhance the prediction of HBV-related ACLF occurrence and outcomes [J]. J Hepatol. 2023;79(5):1159–71.
ARROYO V, MOREAU R. Acute-on-chronic liver failure [J]. N Engl J Med. 2020;382(22):2137–45.
ZANETTO A, PELIZZARO F. Severity of systemic inflammation is the main predictor of ACLF and bleeding in individuals with acutely decompensated cirrhosis [J]. J Hepatol. 2023;78(2):301–11.
WANG N, HE S, ZHENG Y et al. The value of NLR versus MLR in the short-term prognostic assessment of HBV-related acute-on-chronic liver failure [J]. Int Immunopharmacol, 2023, 121(110489.
RICE J, DODGE J L, BAMBHA K M et al. Neutrophil-to-lymphocyte ratio associates independently with mortality in hospitalized patients with cirrhosis [J]. Clin Gastroenterol Hepatol, 2018, 16(11).
ZHANG Y, CHEN P, ZHU X. Lymphocyte-to-white blood cell ratio is associated with outcome in patients with hepatitis B virus-related acute-on-chronic liver failure [J]. World J Gastroenterol. 2023;29(23):3678–87.
JIALAL I, JIALAL G, ADAMS-HUET B. The platelet to high density lipoprotein -cholesterol ratio is a valid biomarker of nascent metabolic syndrome [J]. Diabetes Metab Res Rev. 2021;37(6):e3403.
LU C-F, CANG X-M, LIU W-S, et al. Association between the platelet/high-density lipoprotein cholesterol ratio and nonalcoholic fatty liver disease: results from NHANES 2017–2020 [J]. Lipids Health Dis. 2023;22(1):130.
GINèS P, KRAG A, ABRALDES J G, et al. Liver Cirrhosis [J] Lancet. 2021;398(10308):1359–76.
WANG Z, ZHANG A, YIN Y et al. Clinical prediction of HBV-associated cirrhosis using machine learning based on platelet and bile acids [J]. Clin Chim Acta, 2023, 551(117589.
GRAO-CRUCES E, LOPEZ-ENRIQUEZ S, MARTIN M E et al. High-density lipoproteins and immune response: a review [J]. Int J Biol Macromol, 2022, 195(117 – 23.
CUI B, GUO G, HUI Y, et al. The prognostic value of high-density lipoprotein cholesterol in patients with decompensated cirrhosis: a propensity score matching analysis [J]. J Clin Lipidol. 2022;16(3):325–34.
SARIN SK, CHOUDHURY A, SHARMA M K, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific association for the study of the liver (APASL): an update [J]. Hepatol Int. 2019;13(4):353–90.
HUANG Z, FU Z, HUANG W, et al. Prognostic value of neutrophil-to-lymphocyte ratio in sepsis: a meta-analysis [J]. Am J Emerg Med. 2020;38(3):641–7.
KWON H-M, MOON Y-J, JUNG K-W, et al. Neutrophil-to-lymphocyte ratio is a predictor of early graft dysfunction following living donor liver transplantation [J]. Liver Int. 2019;39(8):1545–56.
LI W, HOU M, DING Z et al. Prognostic Value of Neutrophil-to-Lymphocyte Ratio in Stroke: A Systematic Review and Meta-Analysis [J]. Front Neurol, 2021, 12(686983.
MEI Z, SHI L, WANG B et al. Prognostic role of pretreatment blood neutrophil-to-lymphocyte ratio in advanced cancer survivors: a systematic review and meta-analysis of 66 cohort studies [J]. Cancer Treat Rev, 2017, 58(.
MOREAU N, WITTEBOLE X, FLEURY Y, et al. Neutrophil-to-lymphocyte ratio predicts death in Acute-on-chronic liver failure patients admitted to the Intensive Care Unit: a retrospective cohort study [J]. Shock. 2018;49(4):385–92.
WITTERS P, FRESON K, VERSLYPE C, et al. Review article: blood platelet number and function in chronic liver disease and cirrhosis [J]. Aliment Pharmacol Ther. 2008;27(11):1017–29.
PRADELLA P, BONETTO S. Platelet production and destruction in liver cirrhosis [J]. J Hepatol. 2011;54(5):894–900.
WANG L, XU W, LI X, et al. Long-term prognosis of patients with hepatitis B virus-related acute-on-chronic liver failure: a retrospective study [J]. BMC Gastroenterol. 2022;22(1):162.
LIU C H, LIU S, ZHAO Y B, et al. Development and validation of a nomogram for esophagogastric variceal bleeding in liver cirrhosis: a cohort study in 1099 cases [J]. J Dig Dis. 2022;23(10):597–609.
STøY S, PATEL V C, STURGEON J P, et al. Platelet-leucocyte aggregation is augmented in cirrhosis and further increased by platelet transfusion [J]. Aliment Pharmacol Ther. 2018;47(10):1375–86.
RAPARELLI V, BASILI S, CARNEVALE R, et al. Low-grade endotoxemia and platelet activation in cirrhosis [J]. Hepatology. 2017;65(2):571–81.
NAZIR S, JANKOWSKI V, BENDER G et al. Interaction between high-density lipoproteins and inflammation: function matters more than concentration! [J]. Adv Drug Deliv Rev, 2020, 159(.
TRIEB M, RAINER F. HDL-related biomarkers are robust predictors of survival in patients with chronic liver failure [J]. J Hepatol. 2020;73(1):113–20.
ZHANG Y, CHEN P, ZHANG Y et al. Low high-density lipoprotein cholesterol levels predicting poor outcomes in patients with hepatitis B virus-related acute-on-chronic liver failure [J]. Front Med (Lausanne), 2022, 9(1001411.
MURCH O. Lipoproteins in inflammation and sepsis. I. Basic science [J]. Intensive Care Med. 2007;33(1):13–24.
LI J, LIANG X. Development and validation of a new prognostic score for hepatitis B virus-related acute-on-chronic liver failure [J]. J Hepatol. 2021;75(5):1104–15.
Acknowledgements
We would like to thank the National Natural Science Foundation of China (Grant number: 82360131 and 81960120) and the Postgraduate Innovation Special Foundation of Jiangxi Province (Grant number: YC2023-B058) for financial support. And this work was supported by the Key Laboratory Project of Digestive Diseases in Jiangxi Province (2024SSY06101), and Jiangxi Clinical Research Center for Gastroenterology (20223BCG74011).
Funding
This study was supported by the National Natural Science Foundation of China (grant number: 82360131 and 81960120) and the Postgraduate Innovation Special Foundation of Jiangxi Province (Grant number: YC2023-B058).
Author information
Authors and Affiliations
Contributions
Linxiang Liu and ChenKai Huang contributed equally to this study. Linxiang Liu designed and wrote the original draft, Chenkai Huang analyzed the data and provide interpretations of the results. Yuan Nie analyzed the data, Yue Zhang collected the data and created some of the figures. Juanjuan Zhou and Xuan Zhu critically revised the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the First Affiliated Hospital of Nanchang University (Approval IIT-2021-09). Informed consents of the patients were waived by the Ethics Committee of the First Affiliated Hospital of Nanchang University because of the retrospective and anonymous nature of the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liu, L., Huang, C., Nie, Y. et al. Low platelet to high-density lipoprotein ratio predicts poor short-term prognosis in hepatitis B-related acute-on-chronic liver failure. BMC Infect Dis 24, 888 (2024). https://doi.org/10.1186/s12879-024-09769-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-024-09769-0